Combination Syndrome is seen in a patient with a Single Complete Denture in the maxilla opposing natural mandibular teeth. Let’s read the mechanism
Introduction
The construction of a single denture may involve a variety of dental combinations. A single denture can be constructed against,
- Natural teeth,
- A removable partial denture, or against
- A previously constructed complete denture.

Definition
A single complete denture is a complete denture that occludes upon some or all of the natural teeth, a fixed partial denture, or an earlier formed removable partial denture or a complete denture.
Advantages
The single denture wearer is typically young individuals
Ridges are usually well-formed and
Often, it shows a desirable degree of tissue resiliency.
Seldom there are signs of chronic irritation, hypertrophy, or marked resorption.
Construction and delivery of single complete dentures are more complicated than the delivery of upper and lower complete dentures…
Problems
• The design to articulate and to function with a previously existing occlusal scheme,
• The techniques employed, the problems experienced, the treatment plan and the prognosis vary in various clinical situations.
• It is advisable to consider the numerous clinical sequences separately.
There are four reasons for this increased difficulty,
- The ability of the patient to produce heavy occlusal forces [opposing natural teeth].
2. The unsuitability of the denture foundation tissues (mucosa) to resist high occlusal forces, which results in advanced bone loss.
3. Supra-eruption of the opposing natural teeth creating unharmonious occlusal plane and minimizes the vertical space for setting the opposing denture teeth.
4. Mesial drifting of the opposing natural teeth leading to increase mesial axial angulation (tilting) which produce an unharmonious occlusal plane
Causes of occlusal problems and fracture of denture bases:
1. The position of the mandibular teeth, which may not be probably aligned to achieve bilateral balance for stability.
2. Flexure of the denture base.
Maximizing the ability of denture supporting tissue to withstand destructive occlusal forces
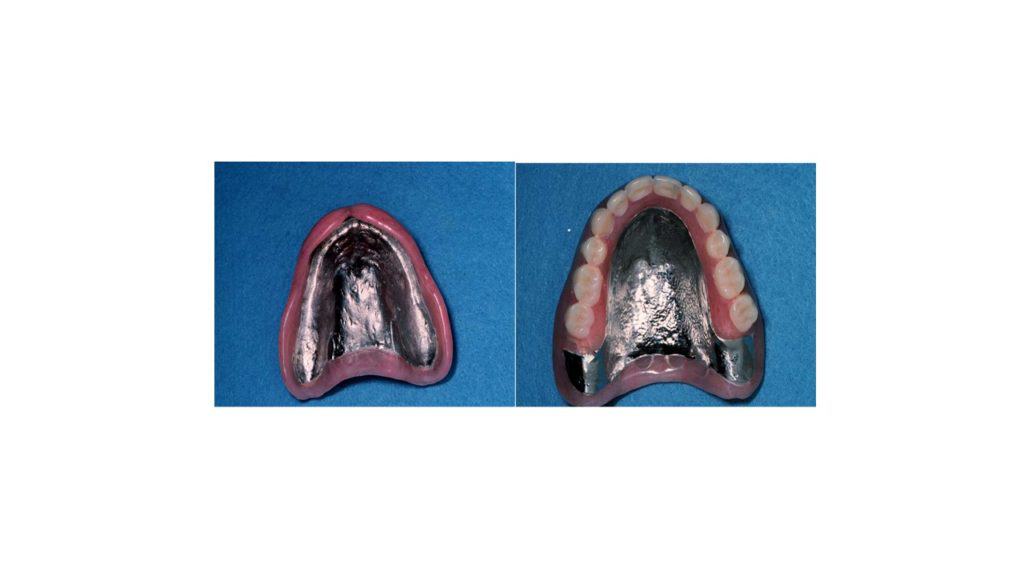
Cast Metal Denture Base, Used if denture fractures repeatedly & the usual causes are,
- Heavy forces from natural teeth
- Occlusal contacts on inclines
- Impingement on a bony midline
- Flexing of the denture
Diagnosis and treatment planning
The primary diagnostic procedures are the same as that of completely edentulous patients. Nevertheless, when only one arch is edentulous, tooth positions in the dentate arch may preclude such purposes. Unfavorable force distributions may then create adverse tissue alterations that compromise optimum function. It is, therefore, important to recognize such clinical changes and to fix them.
These changes include:
(1) Extensive morphological changes in denture foundation causing occlusal plane discrepancies,
(2) Extreme jaw relationship.
(3) Excessively displaceable denture bearing tissue.
A thorough analysis of the remaining teeth should be a primary consideration. Before you proceed with the single denture, there are several factors to be recognized in assessing the teeth in the opposite arch.
In assessing the natural dentition, the following should be reviewed:
Irregular alignment of teeth
• Tipping,
• Extrusion,
• Rotation, etc.
Character of the occlusal surfaces
Natural teeth exhibiting varying steepness of the cusps and/ or associated abrasion and wear.
Cross-bite relationships
A narrow maxilla, in association with a broad mandible, appends complications to the prognosis of the complete denture.
Number and location of opposing teeth
The stability of the upper denture during function is substantially directly proportional to the number of occluding posterior teeth.
Mandibular Denture to Oppose Natural Maxillary Teeth
• Seldom does this condition occur.
• It normally occurs as a consequence of surgical or accidental trauma.
• A case of surgical trauma is the extraction of the mandibular teeth for persons undergoing irradiation therapy for a tumor.
Complicating factors for single mandibular CD opposing natural teeth
- The denture supporting tissues for the complete mandibular denture is relatively small compared to the maxillary supporting tissue.
- The mucosa and submucosa overlying the periostium and bone of the lower ridge are thin. These two reasons are held responsible for resorption of the underlying bone from occlusal forces of the natural teeth.
Solution
- Consider extraction of healthy upper teeth, since long term health of mouth is at stake?
- Stress reduction should be used
- Processed resilient denture liner
- Over-denture
- Implant retained denture
There can be two situations when a complete mandibular denture, opposing maxillary natural teeth is accepted:
When the patient has a class III relationship
This occurs when the mandible of the patient is larger than normal, or the maxilla is smaller than normal.
When the patient has a cleft palate,
Single Complete upper Denture opposing Natural Mandibular Teeth
It is more commonly found in a single mandibular denture. The diagnostic procedures should decide that;
i. There are enough teeth in the mandibular arch,
ii. Periodontal health is fair
iii. There are no missing teeth to be restored;
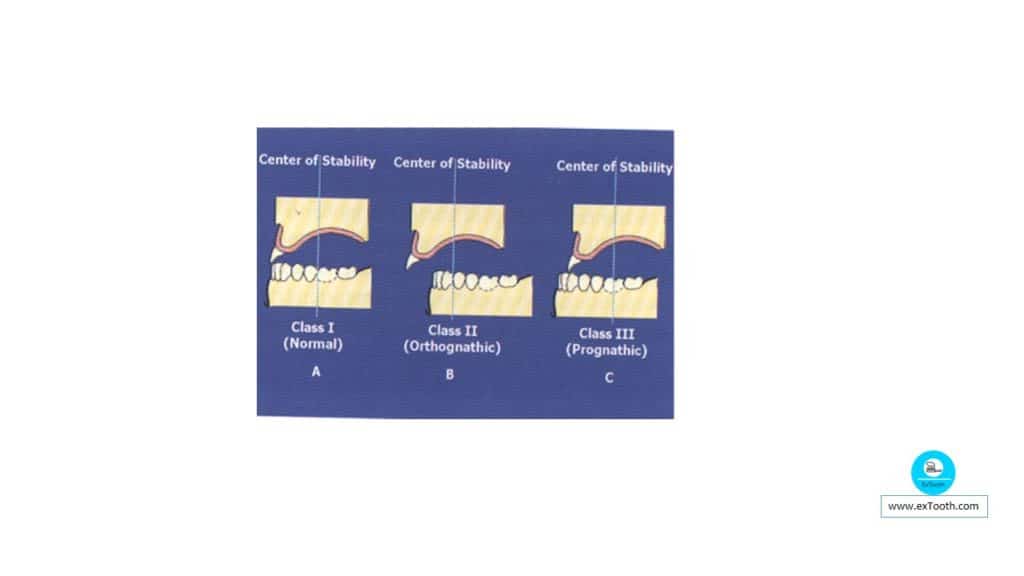
The mandible should have the first molars in jaws with Class I or Class III relation.
In Class II relation, the anterior teeth and premolars bilaterally may serve.
Sometimes the positions of the mandibular anterior teeth don’t allow anterior maxillary teeth to be placed in an esthetically acceptable manner or for balanced occlusion. This situation can be settled as trails:
Rearrange the natural teeth with orthodontic treatment.
Correct the clinical crowns of the teeth by grinding or with restorations.
Affirm balanced occlusion with jaws in centric and not in the eccentric positions.
Avoid a Single Denture against Anterior Teeth Alone, because it results in;
- Resorption
- Loosening
- Fracture
- Combination Syndrome
Solutions;
Fabricate a RPD for Stress Distribution
Make CD & RPD at the same time
Ensures optimal occlusion
Single upper Complete Denture Opposing Natural Mandibular Teeth with a fixed prosthesis
• The problems exhibited are usually in the diagnostic procedures associated with the existing restorations.
• When the restorations are satisfactory, you must then decide what occlusal concept will be continued.
• The same principles of occlusion that implement a complete denture fit to the single complete denture.
Complete maxillary denture to a partially edentulous arch and a removable partial denture;
• The most frequently faced situation for a single complete denture is opposite a partially edentulous arch in which the missing teeth have been or will be replaced with a removable partial denture.
• The partial denture must satisfy the demands of an acceptable prosthesis.
Single Complete Denture Opposing Current Complete Denture
Review of the following five questions should be done before action:
- How long are you wearing existing denture?
- Was the denture constructed at the time of tooth extraction?
- Does the denture meet the obligations of a satisfactory denture?
- Has the denture opposed a complete denture, a partially edentulous arch that held a removable partial denture, restored natural teeth, a fixed partial denture, or natural teeth in which no restorations have been placed?
- Is the operator satisfied to institute CD procedures utilizing the existing denture?
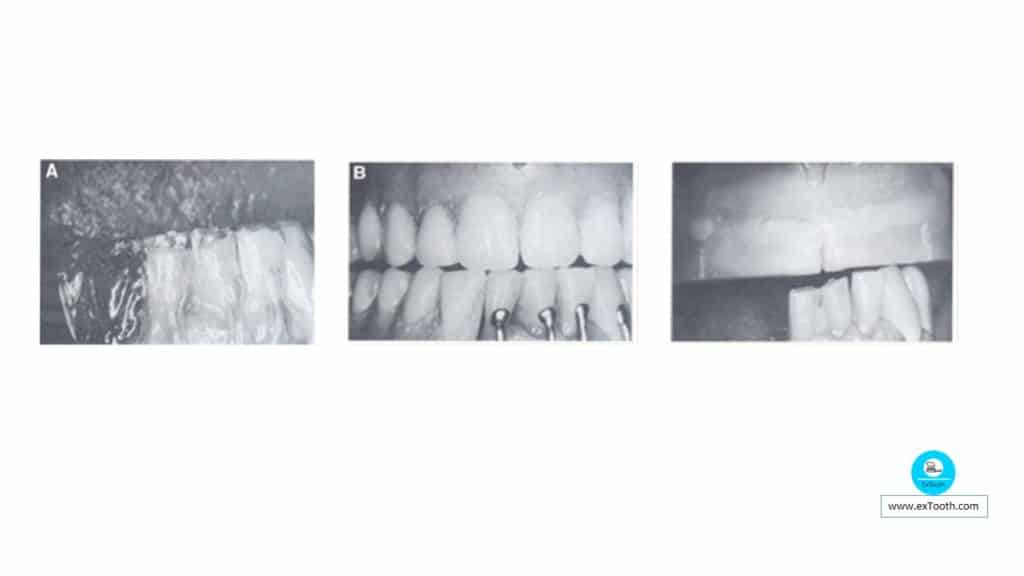
Occlusal adjustment-Perfecting the plane of occlusion:
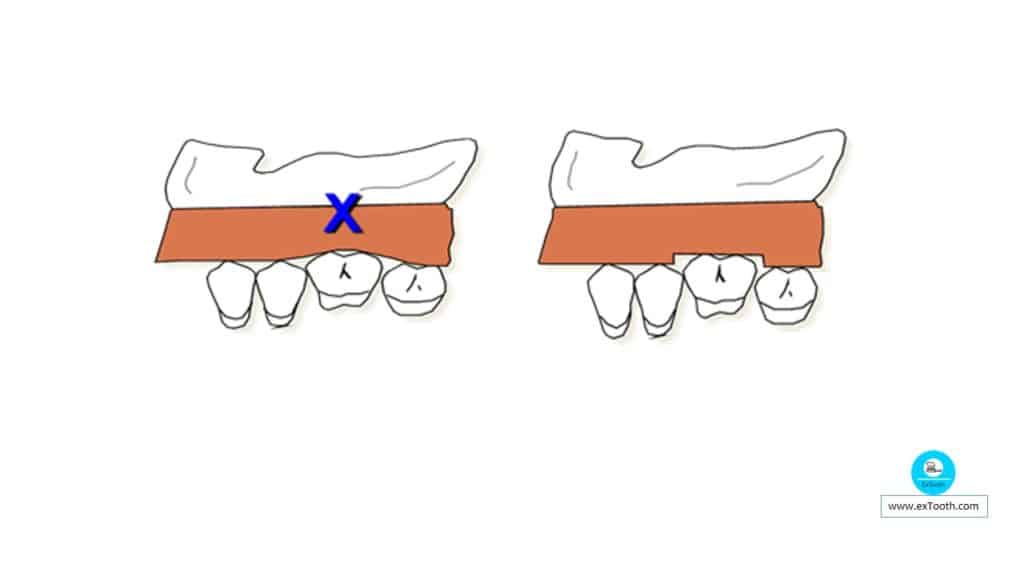
a. Use an occlusal metal template. The inferior surface of the template is slightly convex. The ideal occlusal plane is established when all the incisal edge and occlusal cusps touch this metal occlusal plane resulting in a slightly occlusal plane of the mandibular teeth.
b. The metal template is placed on the incisal and occlusal surfaces of the lower stone cast teeth. Cusps and incisal edges that are too high or too low are identified.
c. The high stone cusps are reduced with sharp knife until there is an even contact of all teeth to the curved occlusal plane template. Reduced areas on the stone teeth are marked on the cast by pencil.
d. The occlusal adjustment is then carried out on the natural teeth in the mouth, using the pencil marked diagnostic cast as a guide.
Impression procedure
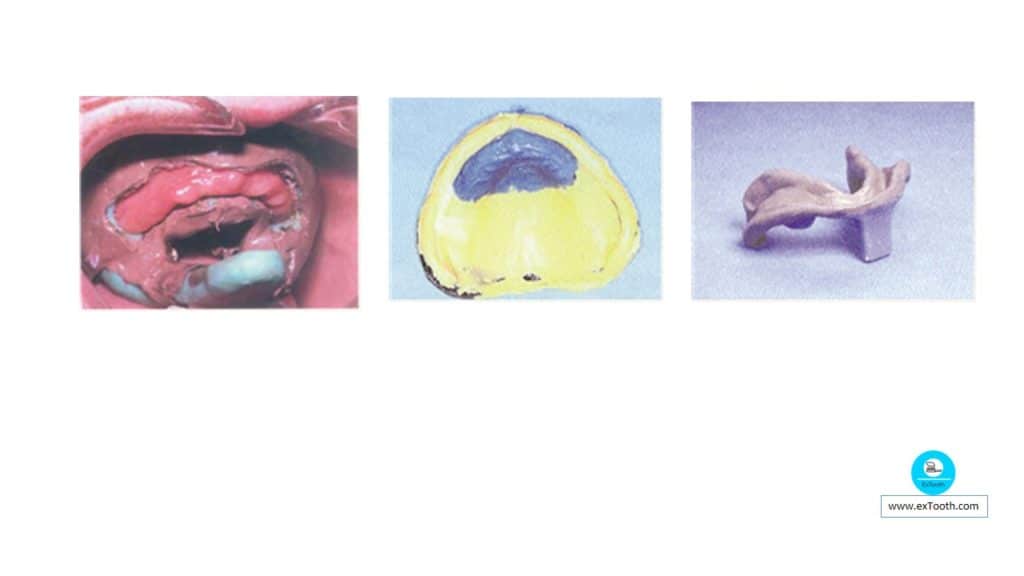
Impression procedure is carried out respecting the clinical situations for maximizing the retentive forces and overcoming the displacing forces. There is commonly readily displaceable tissue in the region of the maxillary anterior ridge. This requires two-stage impressions.
The first step involves developing a peripheral seal, and subsequently, a window is made in the tray corresponding to the area of displaceable tissue. The tray is loaded with medium body polyvinylsiloxane (PVS) and an impression made in the usual way, although the excess material escapes through the window. The tray is then carefully re-seated, and
The second step is performed, which means syringing light-bodied (PVS) through the tray window and over the exposed ridge tissue, to complete the upper impression.
A lower impression was made using the admix technique of greenstick and red impression compounds to take account of atrophic tissues in a mandible opposed by natural teeth.
Impression techniques to overcome the problem of a flabby ridge
1) Watson (window) impression technique
2) Liddlelow technique
3) Osborne technique
4) Lynch and Allen technique
Occlusion Rims;
- Use to establish OVD, & not for Incisal Display
- Overbite will be incorporated when anterior teeth are set, lengthening incisal edges
- Flat Surface for Opposing Teeth
- No inclines.
- If steps in occlusal plane, provide flat areas for opposing natural teeth.
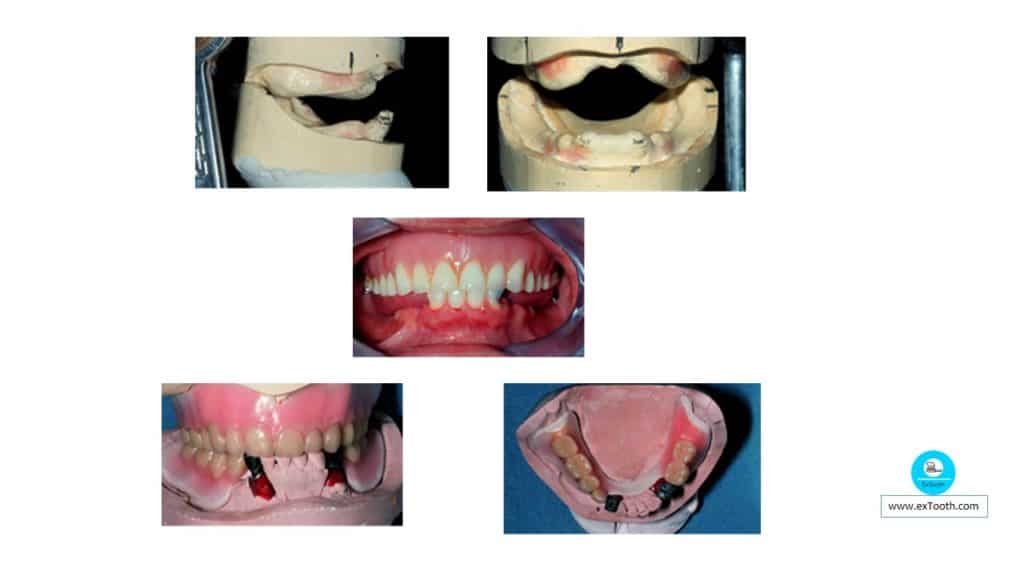
Maxillo-Mandibular Relations
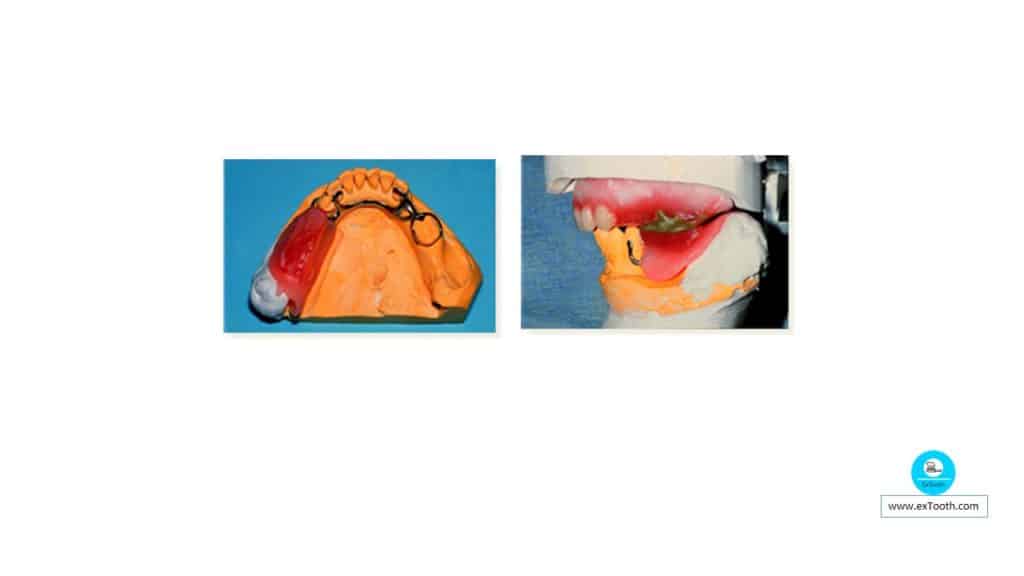
- Occlusion Rims on RPD framework opposes CD Rims.
- Centric and eccentric records with Alluwax Optimizes occlusion.

- Crowns or bridges should be waxed up against the CD tooth setup.
- Optimizes occlusion, ensures changes to be made & then Centric Registration recorded.
Teeth arrangement
Artificial teeth to be used
Occluding surfaces of the teeth and fixed prosthesis made of porcelain; the choice of artificial teeth is porcelain or acrylic resin.
Occlusal surfaces are made using mixed enamel and gold or gold alone; we prefer using gold. However, acrylic resin teeth are fair.
Acrylic resin teeth are picked opposing a prosthesis with the same material
Setting Anterior Teeth
- More difficult
- Setting for esthetics may produce excessive overbite with natural teeth
- Decreases stability
- Compromised position, used to balance need for esthetics & function
Posterior Denture Teeth
- Requires more adjustment to obtain stable centric contacts
- Denture teeth will not normally articulate well with natural dentition
Precautions in Teeth Arrangement
Deep vertical overbite is avoided in the anterior region.
Doing so results in less stress on the anterior teeth and thereby gives improved stability to the completed denture.
Raising the horizontal overjet is one way of decreasing the incisal guide angle.
It is essential that there is no locking in the anterior portion.
Broad surface contacting steep inclined planes must be avoided.
If the opposing teeth have comparatively shallow cusps, then relatively shallow (20 degrees) artificial teeth are elected to articulate with it,
With steep cusps, 33-degree teeth are used, and with flat occlusal surfaces, zero degree teeth are selected.
Classification
The subsequently recommended classification system can explain the identification and treatment of patients.
Class I: patients for whom minor, or no, tooth reduction is all that is needed to obtain balance
Class 2: patients for whom minor additions to the height of the teeth are needed to obtain balance
Class 3: Patients for whom both reductions and additions are needed to achieve balance. The treatment of these patients ordinarily requires a transformation in the vertical dimension of occlusion
Class 4: patients who present with occlusal discrepancies that require addition to the width of the occluding surface
Class 5: patients who present with combination syndrome as described by Kelly
Class I: patients with minor, or no, tooth reduction is all that is needed to obtain balance
Includes patients for whom occlusal adjustments are made to the existing dentition to achieve balance in all excursive movements. Two methods can be used in the laboratory to evaluate the changes that must be made to the teeth.
The first method, described by Swenson, is performed with casts articulated at the correct vertical dimension and maxillary teeth set, one at a time, to an ideal setup. As interferences arise, the opposing teeth on the cast are adjusted to allow for the ideal maxillary tooth positioning.
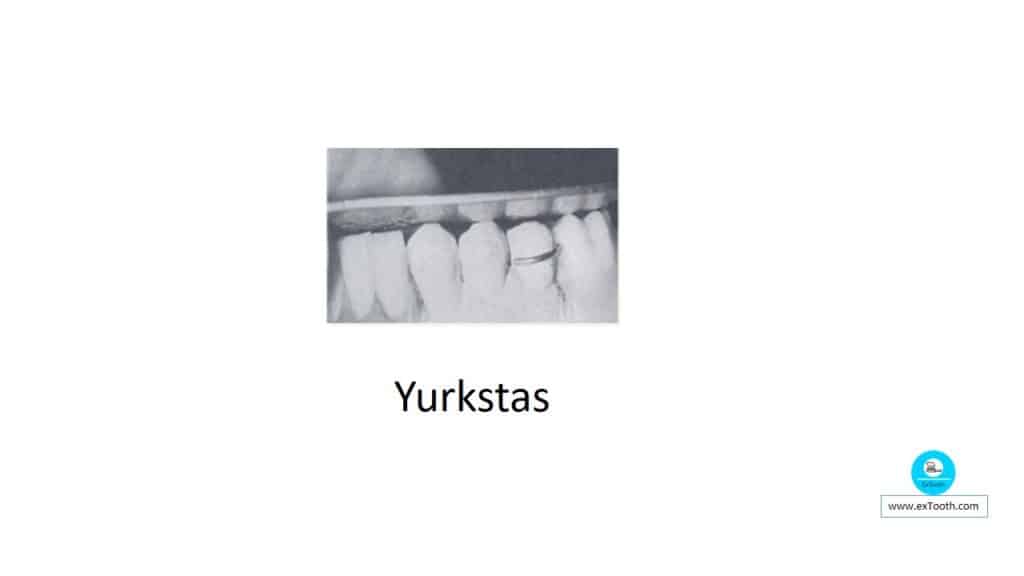
The second method, described by Yurkstas. It involves the use of a curved V-shaped occlusal – metal template that is placed on the incisal and occlusal surfaces to evaluate the potential interferences or areas that are below the plane of occlusion. These areas are adjusted to conform to the curve of the template, and then the denture teeth are set against this plane
Class 2 patients with minor additions to the height of teeth needed to obtain bilateral balance. This situation occurs, when there has been loss of structure because of trauma or decay or when isolated supraeruption in areas without the loss of vertical dimension.
Class 3 includes patients for whom both reductions and additions to teeth are required to obtain balance.
These patients often require restoration of the vertical dimension of occlusion.
Class 4 includes patients whose occlusal discrepancies require addition to the width of the occluding surface
These patients typically have an Angle’s class 2 malocclusion, and present with constricted arches resulting in a posterior crossbite or a with a Brodie bite in which the entire mandibular dentition is lingual to the palatal surfaces of the maxillary teeth
Class 5: patients who present with combination syndrome as described by Kelly
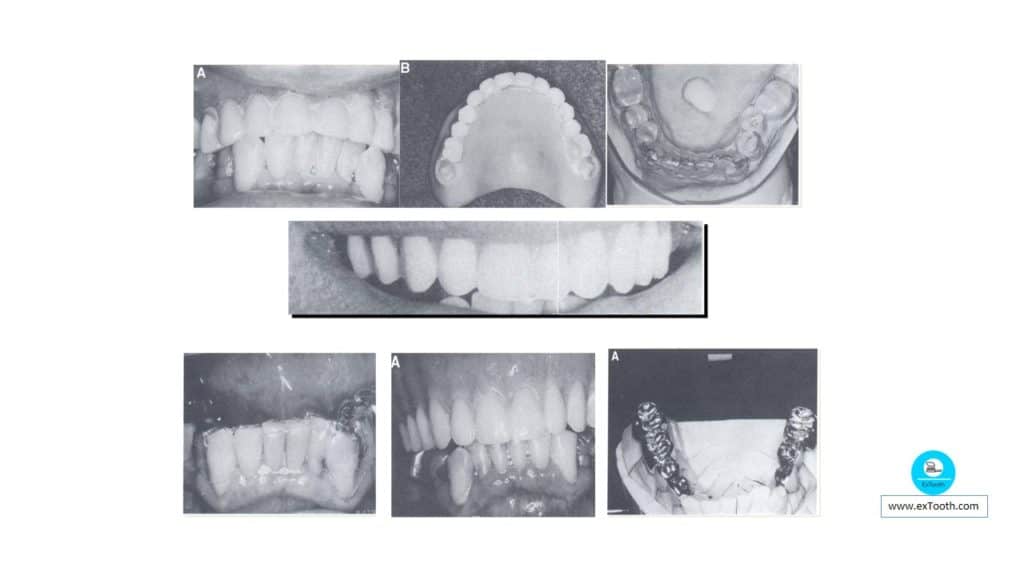
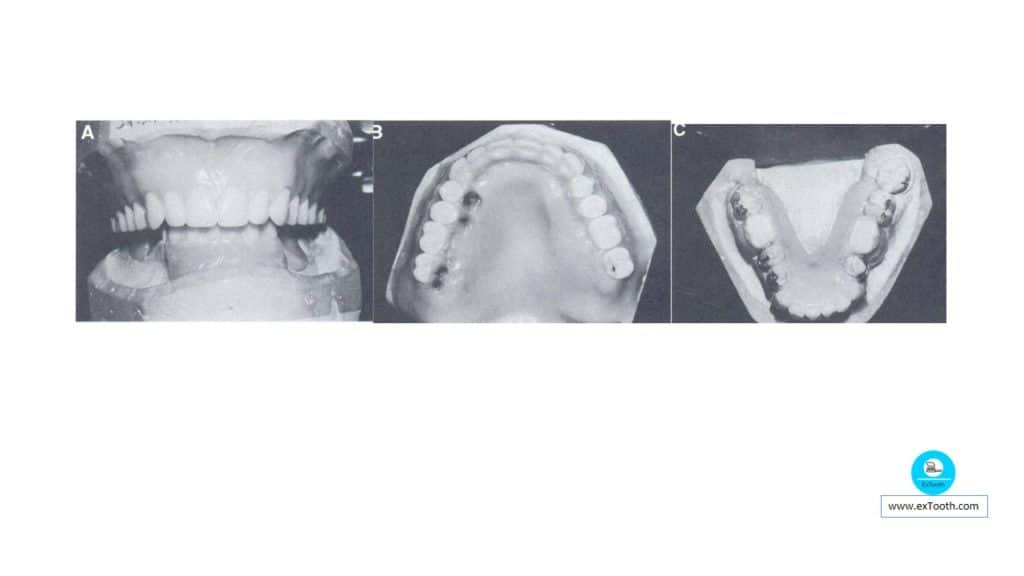
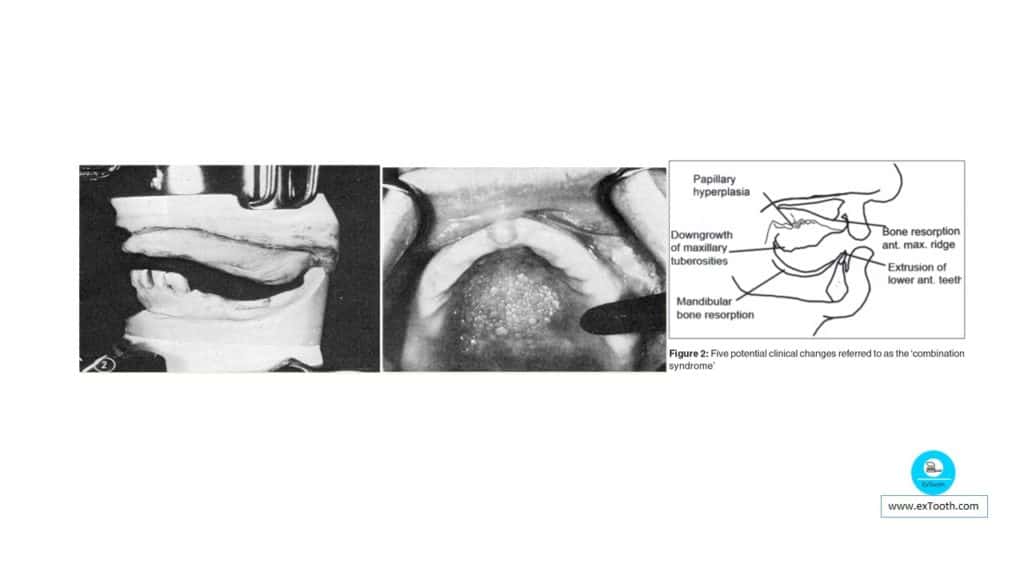
Combination syndrome
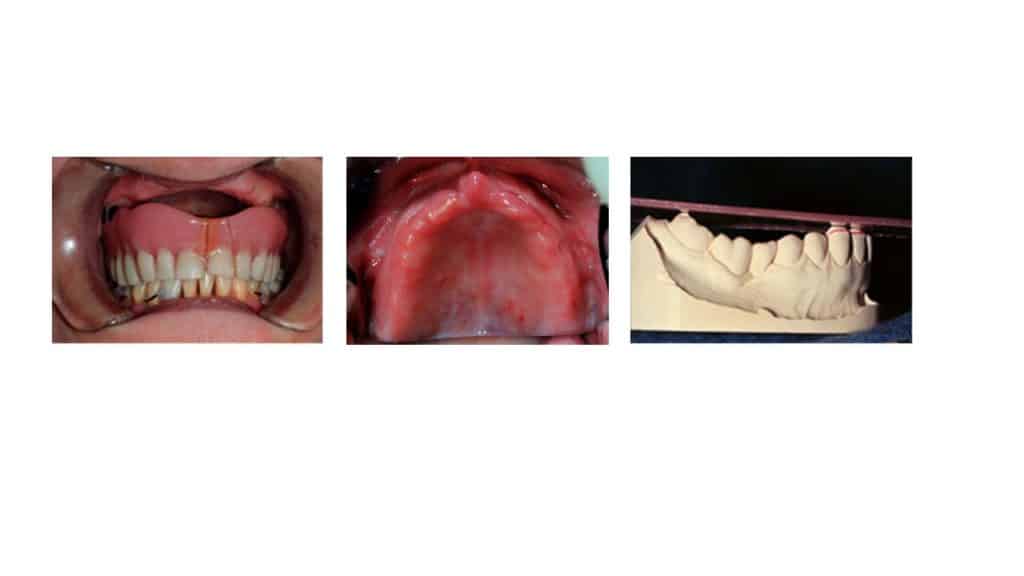
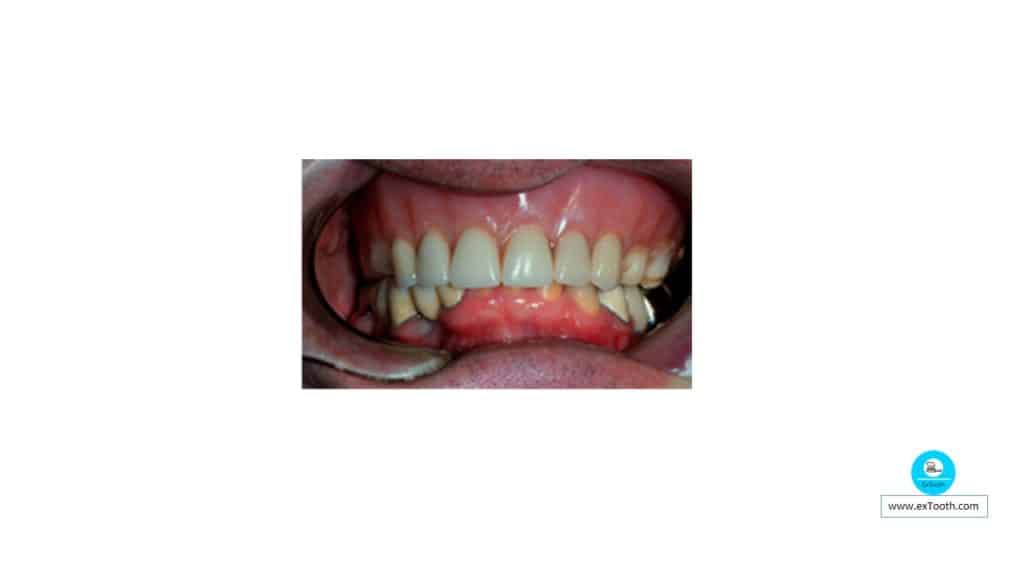
The difficulties confronted by having to give a complete denture in one arch while the opposing arch contains a natural dentition; this challenging clinical combination was termed the combination syndrome by Kelly, with reference to the maxillary arch being edentulous. Also called as “Anterior Hyperfunction Syndrome.”
According to GPT 1 combination syndrome is described as “the characteristic features that occur when an edentulous maxilla is opposed by natural mandibular anterior teeth,
- loss of bone from the anterior portion of the maxillary ridge,
- overgrowth of the tuberosities,
- papillary hyperplasia of the hard palatal mucosa,
- extrusion of mandibular anterior teeth, and
- loss of alveolar bone and ridge height beneath the mandibular removable partial denture bases,
Complete denture opposed by a natural denture was described classically by Tillman in 1961 and Kelly in 1972.
Tillman described the complete lower denture opposed by an upper removable partial denture (RPD), while
Kelly described the opposite scenario.
The latter condition is most prevalent in clinical practice.
Five changes constitute a Combination syndrome. These are quite characteristic
(1) Loss of bone from the anterior part of the maxillary ridge,
(2) Overgrowth of the tuberosity,
(3) Papillary hyperplasia in the hard palate,
(4) Extrusion of the lower anterior teeth, and
(5) The loss of bone under the partial denture bases.
Saunders et al; stated that 6 other changes are commonly associated with this scenario:
• Loss of vertical dimension of occlusion
• Occlusal plane discrepancy
• Anterior spatial repositioning of the mandible
• Poor adaptation of the prostheses
• Epulis fissuratum
• Adverse periodontal changes
To these factors, a seventh factor might also be added, namely the fact that a number of patients may elect not to wear a lower prosthesis, which was provided to provide posterior occlusion. This would appear to be exceptionally true of free-end saddle partial dentures.
Saunders et al; recommended that the essential objective of treatment planning in these cases was “to provide an occlusal scheme that could best discourage excessive occlusal pressures in the maxillary anterior region in both centric and eccentric occlusal contacts”.
Described by Kelly and also reviewed by Lauciello that two methods emerge from the literature to fashion the occlusion:
- A functionally-generated path
- An articulator which has been programmed to reproduce the patient’s mandibular movements.
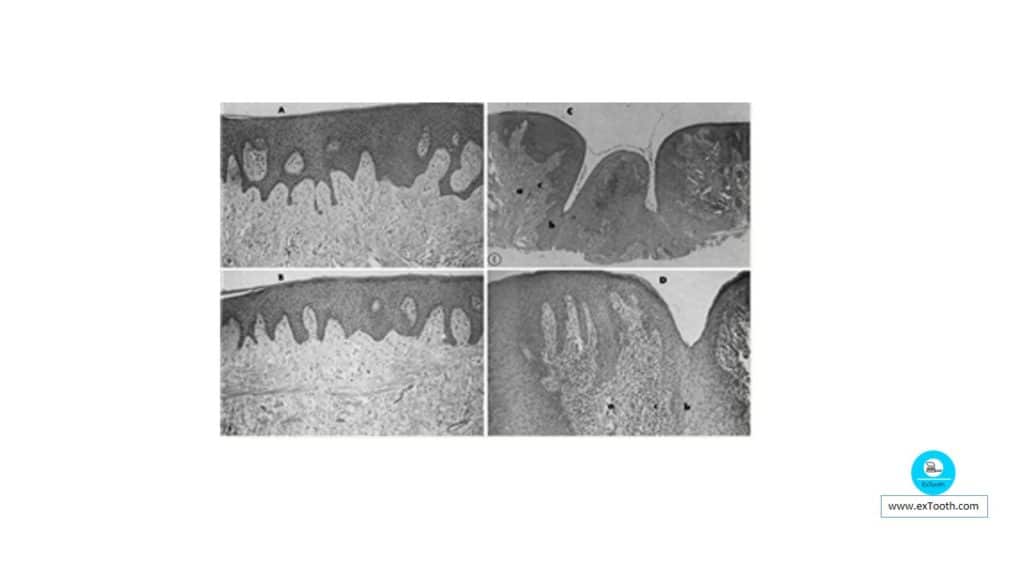
Histopathology of Combination Syndrome
Flabby tissue and the hard tissue over the tuberosity are indistinguishable. They are made up of mature, dense, fibrous connective tissue.
This tissue in both locations has
i. Dense bundles of collagen fibers,
ii. Relatively few cellular elements, &
iii. Very few inflammatory cells.
Mechanics of Combination Syndrome
Kelly’s Hypothesis
Bone resorption in the maxillary anterior region initiates the changes. With the posterior palatal seal, a negative pressure is produced posteriorly to the fulcrum line. This negative pressure may account for the enlarged tuberosity and the papillary hyperplasia.
Carlson observed an increase in the maxillary ridge height in the molar region He postulated: “It may have been due to the development of a fibrous part possibly owing to the suction effect when the denture moved.”
Saunder’s Hypothesis
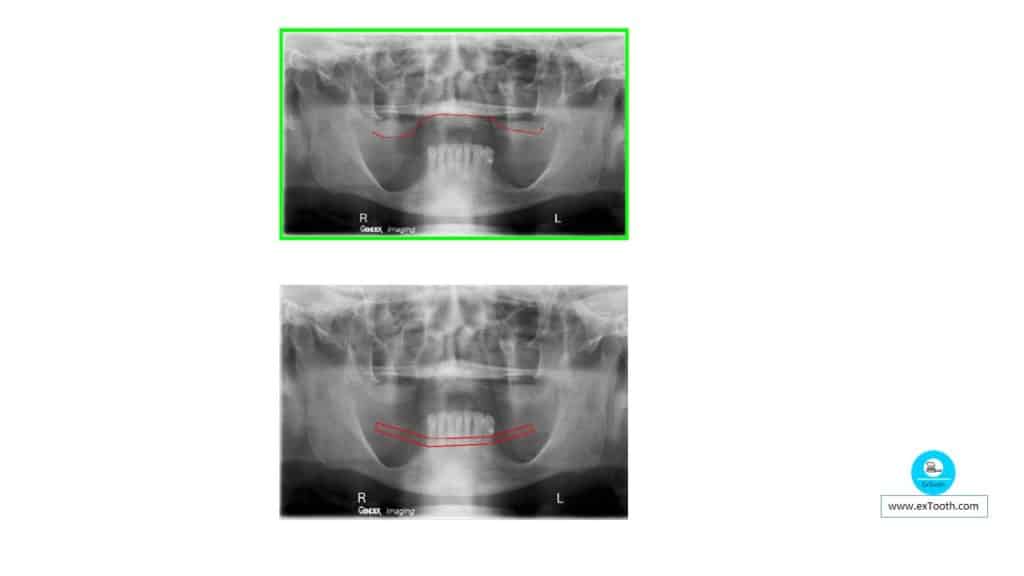
Sequence of events is initiated by the loss of mandibular posterior support, resulting in a gradual decrease of occlusal load posteriorly and an increased occlusal load anteriorly. Eventually, this increased pressure results in resorption of the maxillary anterior ridge.
Prevention of the combination syndrome
- Eliminate the combination of complete upper dentures opposing Class I lower partial dentures by retaining weak posterior teeth as abutments by means of endodontic and periodontic techniques.
- Endosseous endodontic implant
- An overlay denture on the lower
Treatment planning for Combination Syndrome
Strategies for Prevention of resorption
Correction of occlusal discrepancies
a) Reshaping by grinding
b) Providing new restorations
c) Reshaping with RPD framework
Retaining root tips, particularly in the premaxilla, to facilitate support.
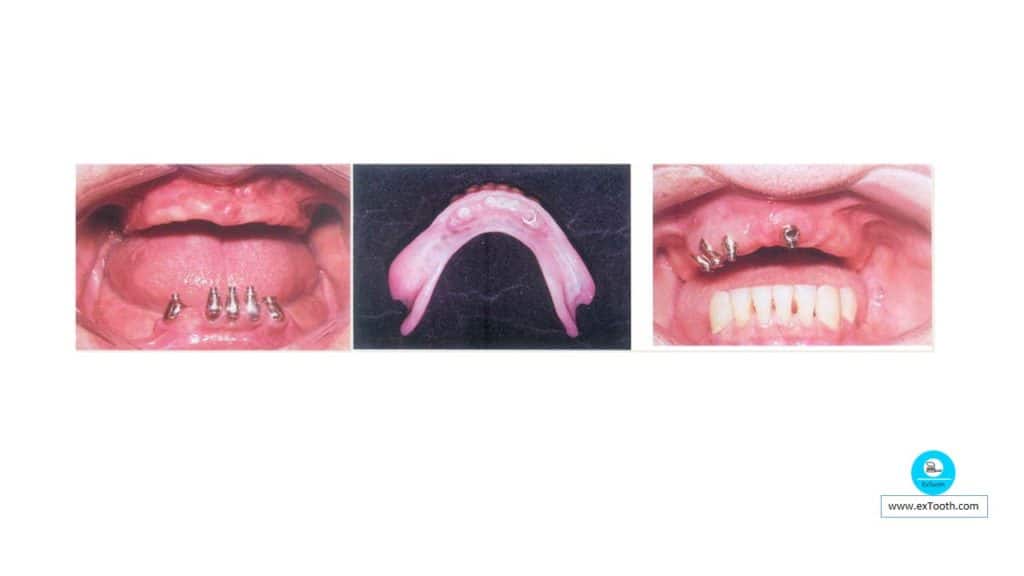
Placing osseointegrated implants to facilitate support
Saunders et al; recommended that the essential objective of treatment planning in these cases was “to provide an occlusal scheme that could best discourage excessive occlusal pressures in the maxillary anterior region in both centric and eccentric occlusal contacts”.
This can be achieved by
• A functionally-generated path
• An articulator programmed to reproduce the patient’s mandibular movements.
Treatment strategies for Combination Syndrome
Two “conventional” approaches are possible here, namely;
- Prosthodontic alone and
- A combination of Prosthodontics and pre-prosthetic surgery.
Prosthodontic treatment alone
Treatment should be endeavored at using a suitable selective pressure impression technique that satisfies prosthodontic patterns. At the next clinical stage, the clinician must decide on the occlusal configuration of the denture. This will involve three related, yet distinct procedures.
The first phase, advocated by Tillman, is to record the relationship of the maxillary occlusal plane to the condylar axis; this requires a face bow transfer.
The second phase is to record appropriate maxillomandibular relations.
One technique useful in these cases is to use a device that allows the production of an arrowhead (gothic arch) tracing.
The third phase relates to what Tillman termed an
“Accurately conceived occlusion”.
Debate exists whether anatomical or non-anatomical teeth should be selected.
Prosthodontic/ pre-prosthetic surgery
Papillary hyperplasia can be reduced, and the enlarged tuberosity can be overcome. This allows the distal end of the occlusal plane to be raised to the proper level and allows the lower partial denture bases to be extended fully.
Placement of osseointegrated implants.
Vestibuloplasty to increase the relative height of the anterior mandible, in addition to minor hard or soft tissue surgery
Conclusion
Constructing a single complete denture is a compact procedure that demands complete knowledge of the basics of denture occlusion. The basic principles of retention, stability, and support should not be taken for granted, and steps must be completed so that all components are working in harmony for the success of the single complete denture. “Dentures & Implants are not a replacement for teeth……They are a replacement for NO teeth.”