SELECTION CRITERIA FOR PONTIC AND PONTIC DESIGNS
INTRODUCTION
Pontic or the artificial crown derives its name from a latin word “Pons” which means bridge.
Pontic serves to restore the mastication, speech to maintain tooth relationships, both interarch and intra arch, and also to satisfy patients esthetic and psychological needs by eliminating the space in dentition.
All the functions should be executed in a manner compatible with oral health and comfort.
Pontic may be connected to a retainer through a rigid connector such as a cast joint or soldered joint or a non-rigid connector such as key and keyway or as in telescopic retainer.
- Replaces lost natural tooth
- Restores function
- Occupies missing space acts as space maintainer.
- Though when pontic was first designed or used is unknown, history of pontic dates way back to 1918 when Tinker proposed hygienic pontic.
- In 1930 conical pontic was introduced.
- Ovate pontic was designed by Deeway and Lugsmith in 1933.
- Stein 1966 introduced Egg-shaped pontic.
- Perel in 1972 presented modified sanitary pontic.
- Belorend introduced multiple fused pontics in 1981.
- Shoher and Whiteman introduced Inzoma pontic in 1983.
Definition
Glossary of Prosthodontic Terms ( GPT– No. 7)
Pontic is defined as an artificial tooth on a fixed partial denture that replaces a missing natural tooth, restores its function and usually fills the space previously occupied by the clinical crown.
CLASSIFICATION
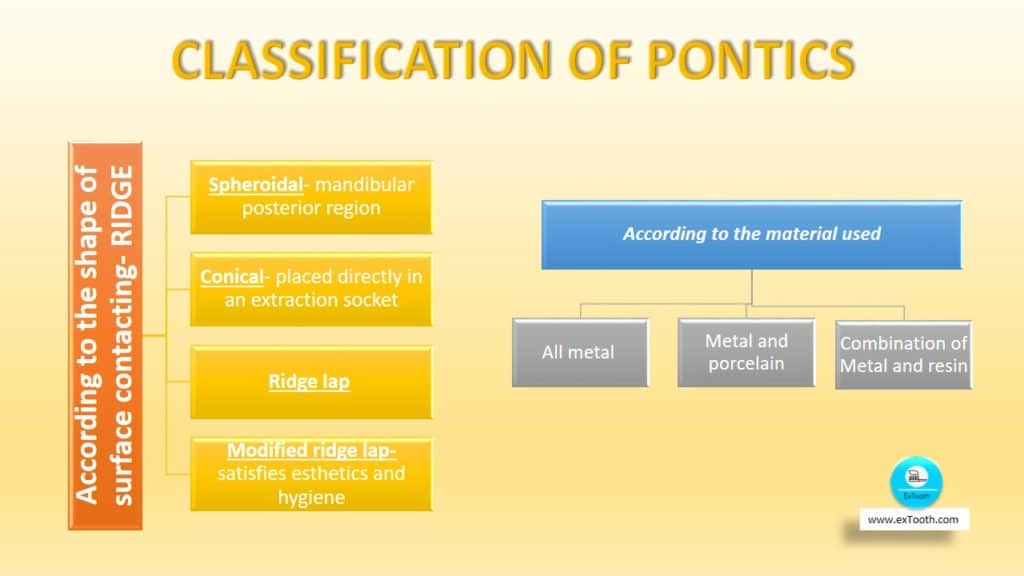
According to the shape of surface contacting- RIDGE
Spheroidal- mandibular posterior region
Conical- placed directly in an extraction socket
Ridge lap
Modified ridge lap- satisfies esthetics and hygiene
According to the material used
All metal
Metal and porcelain
Combination of Metal and resin
According to the pontic facing by manufacturers
Prefabricated facings
1. Flat back interchangeable facing
2. Trupontics
3. Pontips- dentist desiring glazed porcelain in contact with residual ridge
4. Long pin facing
5. Reverse pin facing
Custom made pontics (Facings):
1. Porcelain fused to metal
2. Acrylic facing
Basic requirements
Restore function
Good esthetics
Biologically acceptable
Effective oral hygiene
Preserves underlying residual mucosa
Basic philosophy behind fabricating a pontic is that it substitutes natural tooth form, function and appearance. Changes in residual ridge, opposing occlusion and proximal space affect the success of the restoration.
- With time laps after extraction, the space available for the pontic may be compromised because of tooth migration adjacent to the edentulous space. In such cases, abutment teeth are repositioned orthodontically or modification of abutment teeth with complete coverage retainers are done.
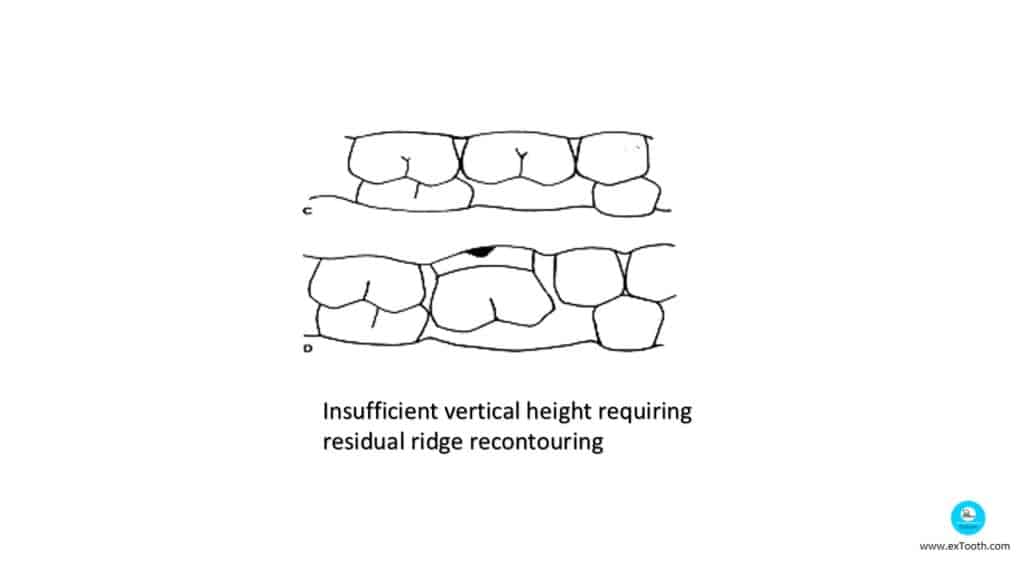
- An attempt to replace with a smaller pontic will compromise esthetics and hygiene. When the vertical height is insufficient, the residual ridge is lowered and reshaped to allow space for physiologic pontic.
- Occlusal plane correction is done before the fabrication of the fixed prosthesis as in the case of supra eruption of opposing teeth.
- Traumatic extraction results in severe bone resorption, surgical ridge augmentation, and soft tissue correction enhance esthetics.
- Thus a thorough consideration and implementation of above said will contribute towards the successful design of a pontic
Basis for design criteria for pontic
- Majority of researchers believe that inflammation of alveolar mucosa under pontic is caused by the accumulation of plaque on the basal surface – Stein R S (1966)
- Podshadley and stein (1968) contradicting didn’t find any relevance between soft tissues and pontic fabricated from gold alloys ,resins gazed ceramics .
- According to Eissmann (1971) The boundaries of edentulous space are residual ridge opposing occlusal surface, proximal surface of abutment teeth and musculature of tongue and cheek or lips.
Substitutes natural tooth form, function and appearance.
Changes in the residual ridge, opposing occlusion and proximal space affect the success of the restoration.
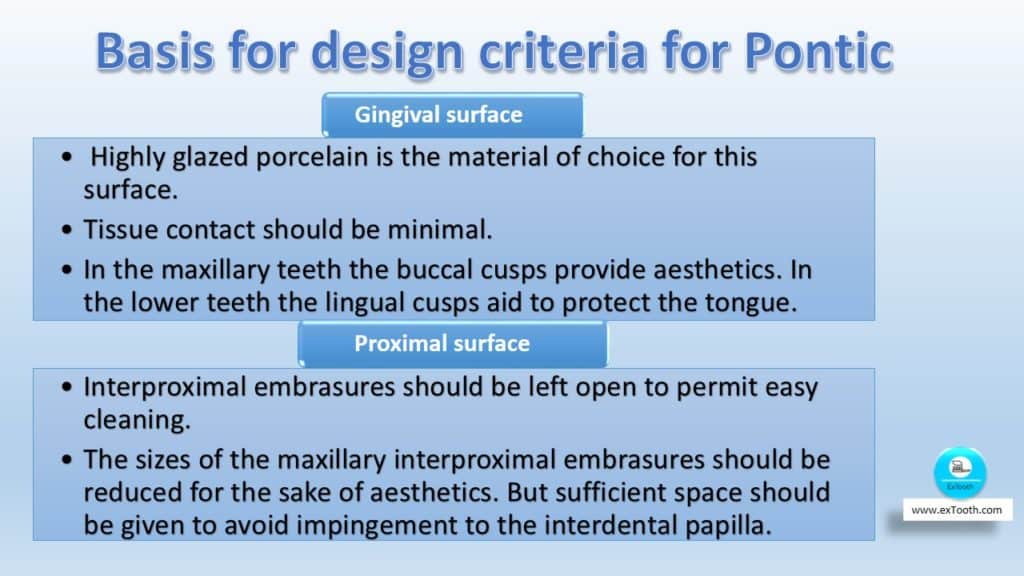
Gingival surface :
- The gingival surface is the most interesting aspect of the pontic design. The material used and the degree of tissue contact affect the success of the restoration.
Tissue contact should pertain to the crest of the ridge. If it is placed more anteriorly, food accumulation may occur
- Highly glazed porcelain is the material of choice for this surface. But studies have shown that the finish of the surface is more important than the material used in maintaining tissue health.
- Tissue contact is very important for a pontic. The pontic should not be designed to pressurize the alveolar mucosa, as it may ulcerate. Tissue contact should be minimal. Hygiene maintenance (flossing) is more important than the pontic design itself.
The pontic should have minimal facial contact to obtain good tissue response. If the contact ‘is extended onto the alveolar mucosa, severe ulceration may be produced
- The functional cusp is the load-bearing cusp of the tooth.
- In the maxillary teeth the buccal cusps provide aesthetics. In the lower teeth the lingual cusps aid to protect the tongue.
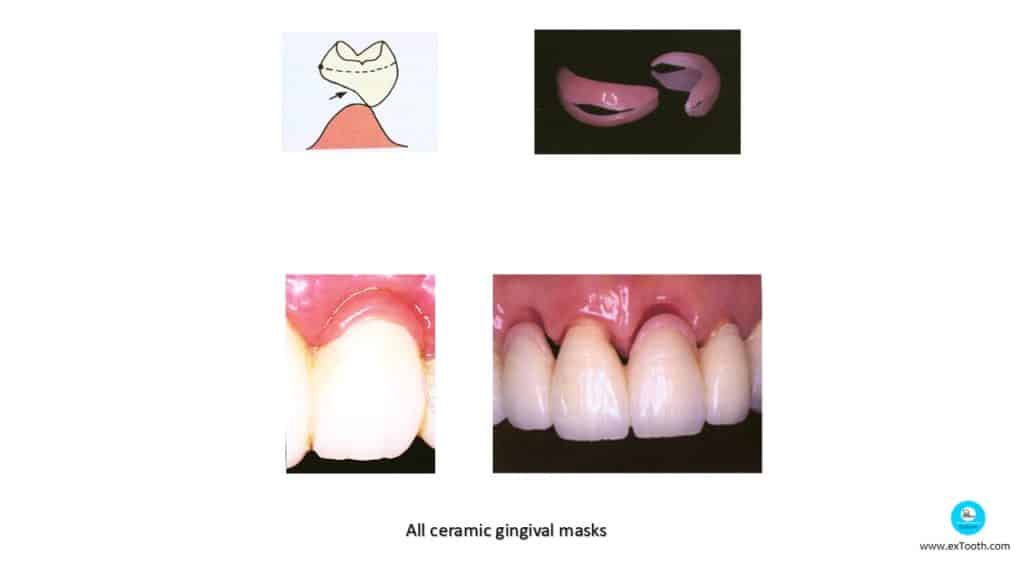
All ceramic gingival masks made of pressed glass ceramics
All ceramic gingival masks
Local alveolar ridges defects masked with ceramic veneering materials placed on pontics of an anterior FPD.
Proximal surface:
The sizes of the maxillary interproximal embrasures should be reduced for the sake of aesthetics. But sufficient space should be given to avoid impingement to the interdental papilla.
Wider embrasures are provided for posterior teeth for better cleansing. The mandibular molars are provided with large embrasures for better cleaning and aesthetics is not critical.
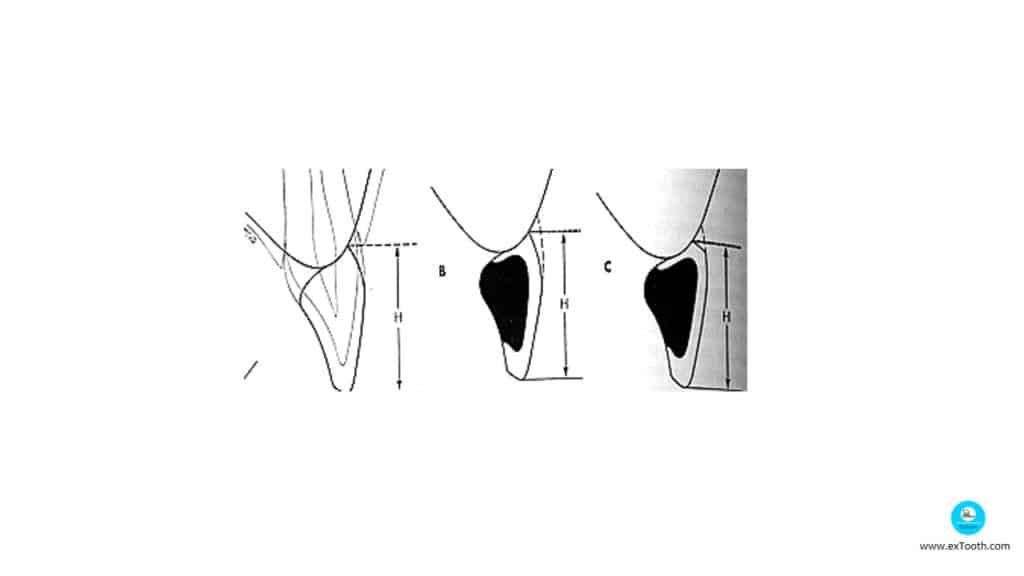
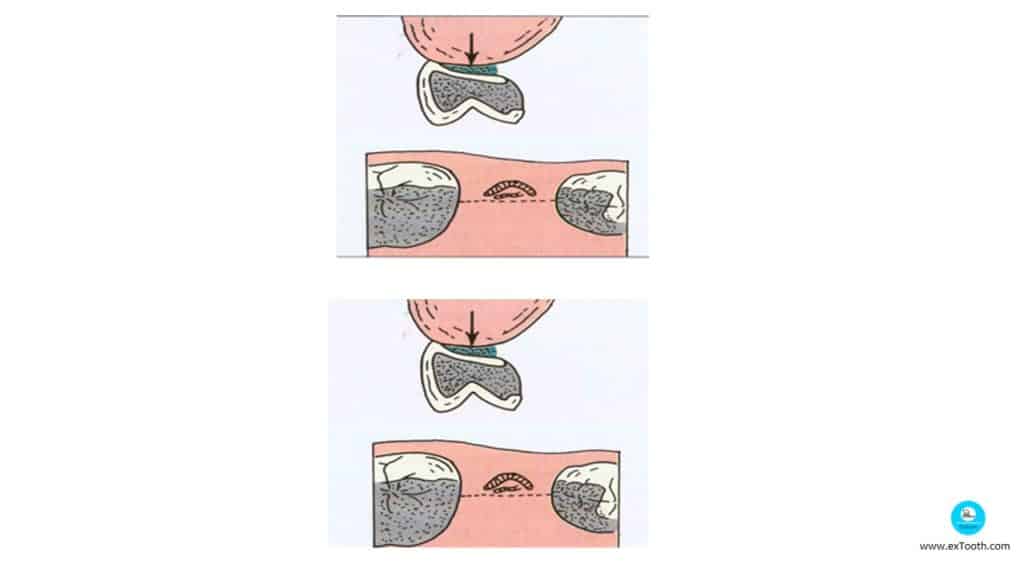
A- Same inciso gingival height
B- correctly contoured pontic
C- incorrect contour.
Buccal and lingual surfaces :
The design is based on the aesthetic, functional and hygienic requirements.
- The facial surface should be designed with aesthetics as the primary concern. It should resemble the adjacent teeth.
- The lingual surface is designed with hygiene as the primary concern.
- The embrasures are wider lingually than facially
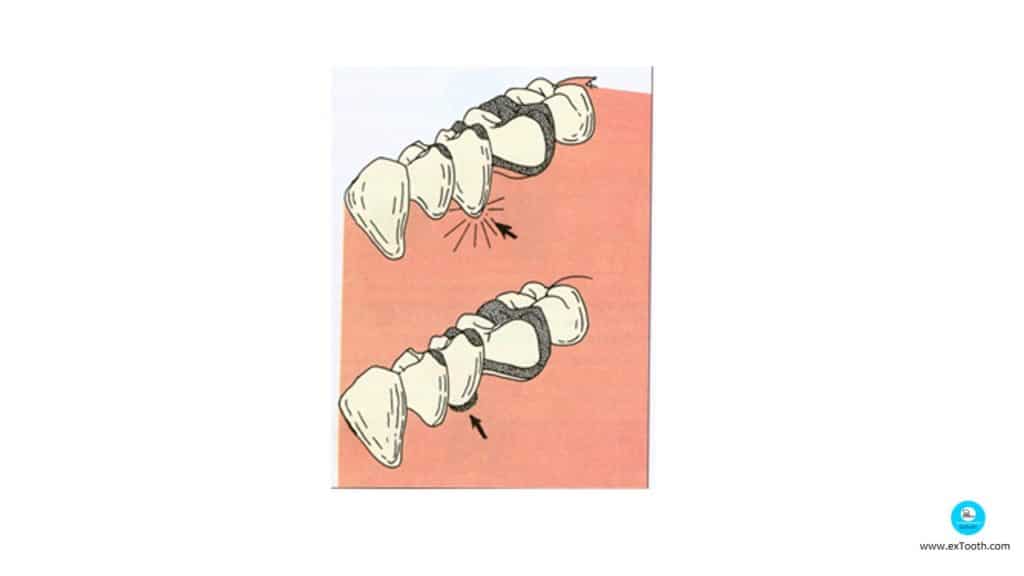
Contour of three pontic shapes

The lingual surface should be designed such that it is similar to adjacent teeth from the cusp tip till the height of contour, then it should recede sharply and concavely from the height of contour towards the facial surface to form a pinpoint contact on the labial surface of the residual alveolar ridge
Principles of designing the framework
1.Should provide uniform veneer of porcelain of approximately 1.2mm. Excess may lead to inadequate support and fracture.
2.Metal surface must be smooth and free of pits – else may lead to incomplete bonding of porcelain.
3.Sharp angles should be avoided to prevent stress concentrations.
4.Occlusal contacts must be placed so as to avoid metal porcelain fracture during centric and eccentric movements and contacts.
Edentulous space
The space created due to the loss of a tooth is usually sufficient for the fabrication of a good pontic. But in many cases, due to a long period of edentulousness, the adjacent teeth tend to be tilted or drifted towards this space. In such cases, a proper pontic cannot be placed and the design of the pontic should be compromised.
- Fabrication of a small anterior pontic gives an ugly appearance. In posterior teeth, small pontics tend to collect more food debris and hence is very difficult to maintain hygiene.
For cases with deficient pontic space, the following procedures can be done:
- Orthodontic movement of adjacent teeth.
- Placement of modified full coverage retainers.
- Residual ridge contour
- During treatment planning, the diagnostic cast should be thoroughly examined. The contour of the ridge and texture of the soft tissues should be observed during intra-oral examination.
- A smooth rounded ridge is best for the placement of a pontic. In cases with overhanging hyperplastic tissues, surgical excision of these issues should be carried out. Cases with severe residual alveolar ridge resorption should be treated with ridge augmentation, tissue grafts, etc.
Ridge Deformities
According to Siebert
- Class I : Loss of faciolingual ridge width,with normal apricocoronal height.
- Class II : Loss of ridge height, with normal width.
- Class III : Loss of both ridge width and height.
with minimal deformities.
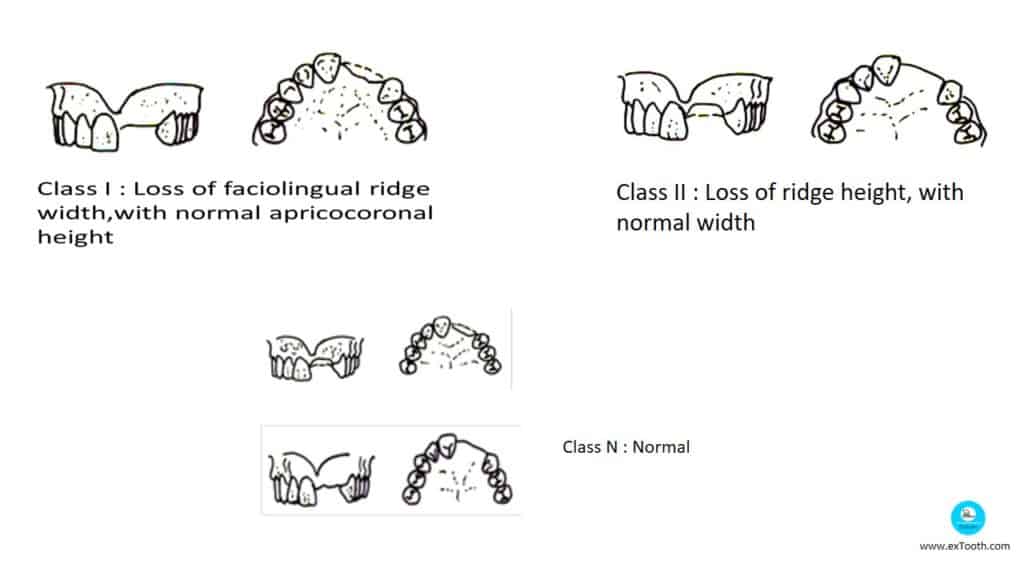
Adams et al in his study showed that 32.4% showed Class I defect, 2.9% Class II, 55.9% being Class III and 8.8% having no defect or Class N.
- In 1987 Abrams H et al in a retrospective study of partially edentulous patient showed that 91% of edentulous anterior section – Alveolar defects .
- In 1983 Seivert gave a suitable classification for alveolar ridge defects.
- After tooth loss, residual ridge is formed from the gingiva and alveolar mucosa-Pontic positioned away from movable mucosa
Treatment planning is done by the study cast and radiograph-To analyze alveolar ridge, abutment teeth, gingiva, size of edentulous space.
Occlusal load on the pontic:
According to Stein, “the basic requirement of a pontic is that it should be able to restore proper function”. The amount of Occlusal load determines the selection of material as well as the design of the FPD.
The functional relationship of the cusps of the pontic and the opposing teeth is the most critical consideration in the design of the pontic
Retainers:
– When PFM retainers are used PFM pontics are selected.
– When partial veneer retainers are used, prefabricated facings are indicated using same metal as retainers.
– If complete metal retainers are used – all metal pontic.
Esthetics:
– Anterior segment – modified ridge lap is the design of choice, as esthetics influences the pontic design.
– Maxillary posterior region –if esthetics a prime consideration modified ridge lap is used with porcelain facing.
– Mandibular posterior region – spheroidal pontic – Patient require an accommodation period for all ceramic FPDs.
Occlusogingival Height and mesiodistal width of edentulous space:
PFM ridge in long span with reduced occlusogingival height can result in porcelain fracture.
If mesiodistal width is reduced, metal pontic with porcelain or acrylic facing is advised.
Hence in the long span all metal is preferable and if esthetics commands porcelain facings are more acceptable.
Amount of Ridge Resorption and Contour:
– They determine tissue contact and clearance.
– 3mm of clearance is recommended for hygiene reasons.
– Recontouring and ridge augmentation in case of large ridge defects.
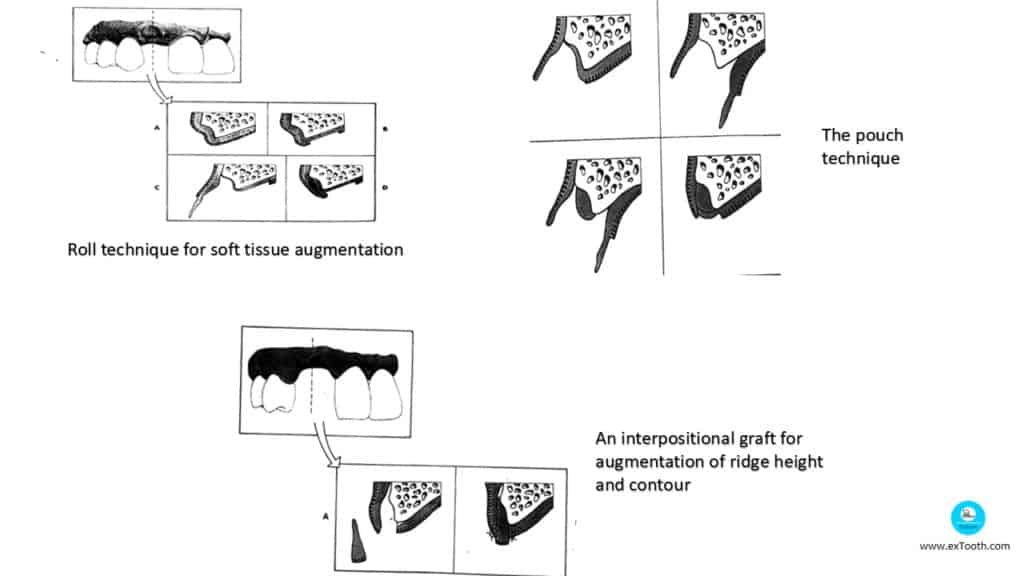
Surgical Correction
- Ridge augmentation is accomplished by addition of either soft or hard tissue, although filling defect with bone is not essential.
- Excellent class I defect is corrected by subepithelial or submucosal graft.
Design considerations for an anterior pontic
- Contact with the labial slope of the ridge should be minimal (pin point) and pressure free (modified ridge lap design).
- A larger contact with the ridge is provided for a natural look. If a pinpoint contact is given for a case with ridge resorption, unaesthetic black spaces may become visible.
- Lingual contour should be in harmony with that of the adjacent teeth.
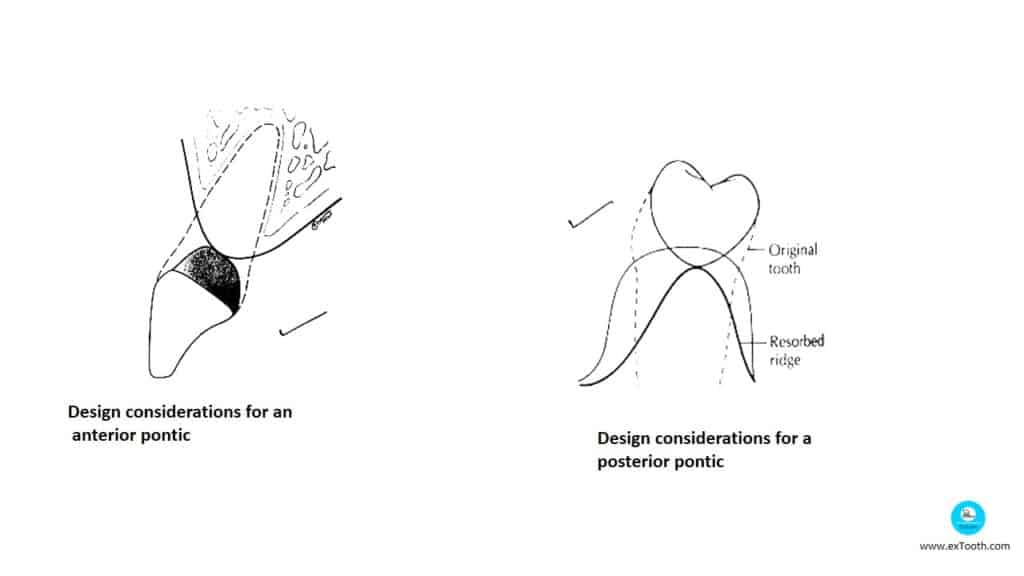
Design considerations for a posterior pontic
- A correctly designed posterior pontic should have the following characteristics.
- Contact with the buccal slope of the ridge should be minimal (pin point) and pressure-free (modified ridge lap design-discussed later)
Design considerations for a posterior pontic
- The occlusion of all the other teeth.
- The buccal and lingual shunting mechanism should correspond to the adjacent teeth.
- The overall length of the buccal surface should be equal to that of the adjacent abutments or pontics
- Cemento-enamel junction of abutment tooth/ teeth used as vertical reference points.
- For esthetics and functional reasons-tooth are harmoniously integrated both horizontally (Lip support) and vertically.
- With time-lapse after extraction, there is a migration of adjacent and opposing teeth – they should be orthodontically repositioned and modified with complete coverage. Smaller pontic will compromise esthetics and hygiene.
- When vertical height is insufficient, residual ridge is contoured is reshaped.
- Occlusal plane correction is done before the fabrication of fixed prosthesis.
Prosthetic soft tissue conditioning –
- In this treatment phase, reliable long term provisional restorations play an important role in determining the contact area of pontic and in remodeling the soft tissue recipient site.
- Therefore mentioned measures taken for soft tissue conditioning are repeated at intervals of 2 weeks until satisfactory contour and pseudo/papillae are formed.
- Soft tissue being contoured by relining the base of long term provisional restoration.
- Long term provisional restorations must be used for a period of 6 to 12 months.
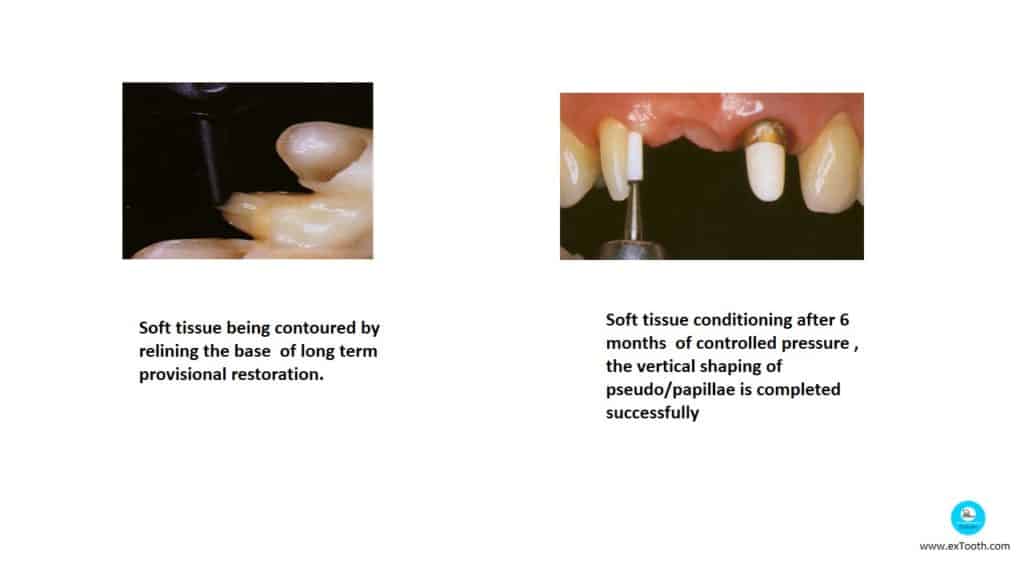
Soft tissue conditioning after 6 months of controlled pressure, the vertical shaping of pseudo/papillae is completed successfully.
Gingival Coloured Ceramics, masks, prosthesis If augmentative measures are contraindicative or undesirable, small alveolar deficiencies and missing papillae can be reconstructed by restorative measures- all gingival ceramic masks
The basal surface must demonstrate a convex shape similar to the ovate pontic design for dental floss – tight contact .
Gingival colored prosthesis is a solution for correcting large alveolar defects associated with esthetics and phonetic problems
Pontic Design Selection
- The retainers
- Esthetics
- Occlusal gingival height and mesio distal width of edentulous area
- Ridge resorption and contour
The success of a fixed partial denture depends on the proper design of the pontic. If the pontic is not designed to restore function and aesthetics, the chances of failure are dramatically increased
Factors Affecting the Design of a Pontic
- The major factors that determine the design of a pontic are:
- Space available for the placement of the pontic.
- The contour of the residual alveolar ridge.
- Amount of Occlusal load that is anticipated for that patient
Review of literature
Arlon G. (1968) studied the effect of various pontic materials on gingiva.
Gingival response to pontic: JPD 1968 (19)
The result after 6 months of observation showed that,
a) all pontics materials tested produced some change when they were in contact with the gingival tissue,
b) All pontic material listed were equally well tolerated by tissue after 6 month interval.
The materials tested were glazed porcelain, unglazed porcelain, acrylic resin and gold.
Roughness of pontic material and dental plaque – JPD 1990 (23) 407-411.
Joseph et al (1990) studied the relationship between surface roughness of the pontics and dental plaque accumulation.
Pontic materials used were glazed porcelain, acrylic resin and cast gold. Clinical results showed that plaque formation was noticed in all the pontic materials used.
Roughness of pontic material and dental plaque – JPD 1990 (23) 407-411.
The authors concluded that, whatever material used maybe and are smoothened as much as possible, they must be cleaned regularly.
Design of multiple pontics – JPD 1981 (46) 634-636.
Donald A. stated that, the fused multiple pontics design, which was thought to be best for mandibular posterior segment can be used in other parts of mouth also.
The interpontic embrasure in filled in anterior segment using pink porcelain which also solves the esthetic problem and in cases of moderate ridge resorption and loss of papillae between pontic and abutment.
Anterior pontic design – JPD 1984 (51): 774-76.
Charles B. Porter, described fixed partial denture with multiple pontics by restricting the pontic embrasure for lower anterior segment. He justified that, the esthetics will not be compromised as in 90% of the cases, the mandibular cervical region is not visible.
Anterior pontic design – JPD 1984 (51): 774-76.
He also showed that, plaque accumulation and calculus deposition are eliminated and no: of surfaces the patient must clean is reduced and maintaining oral hygiene is simplified.
He also suggested this design for posterior segment
Stabilization of Long-span Pontics
Cary P. et al in 1997 derived a simplified techniques for stabilization of the pontics.
Procedure:
1. Prepare a working cast in the usual manner.
2. Drill a hole just lingual to the crest of the edentulous ridge where the pontic will be placed. The hole should not interfere with the pontic tissue contact area.
3. Place a post into the hole and should be seated snugly in the shaft to ensure there is no movement towards the ridge.
4. Cut the other end of the post so it does not interfere with the occlusion, otherwise leave it as long as possible.
5. Wax the abutment retainers and pontic to full contour as usual and incorporate the exposed part of the post into the pontic. Create appropriate proximal contact areas between the pontic and retainer.
6. If veneer is to be applied cut back the wax pattern approximately.
- Finish the margins of the retainer.
- Pontic may be attached to one or more retainers or cast separately and soldered.
- Attach sprue, invest, cast and finish as normal, the post is removed during finishing stage, after the pontic is attached to the retainers.
In the case of a long-span bridge, A technique derived by Ruhlam et al 1967 may be advanced. The technique is similar to that of one described earlier, but individual stabilizing holes are drilled and posts erected for each pontic.
A paralleling drill press is used for drilling the hole, as there holes should be parallel to one another and again parallel to path of insertion and removal. Castings are done in usual manner the pontics are either cast connected or soldered.
Pontic Design Types
- Spheroidal Pontic
- Egg-shaped or Bullet shaped
- Sanitary or hygiene Pontic
- Modified Hygienic Pontic
- Modified Ridge Lap
- Ridge Lap
- Root Extension Type
- Conical Pontic
- Ovate Pontic
- Prefabricated Porcelain Facing
- Plain Long Pin Pontic
- Tru Pontic
- Harmony Facing
- Reverse Pin Facing
- Resin Veneered Pontic
- All Metal Pontics
- Metal Ceramic Pontic
- Aluminous Porcelain Pontics
Spheroidal Pontic
Design of choice in mandibular posterior region
Indicated when we foresee an alteration in ridge contour
Features
1.Contacts the ridge without pressure.
2.Buccal and lingual surface follow a normal tooth form from cusp tip to height of contour and tapers from here to gingival surface.
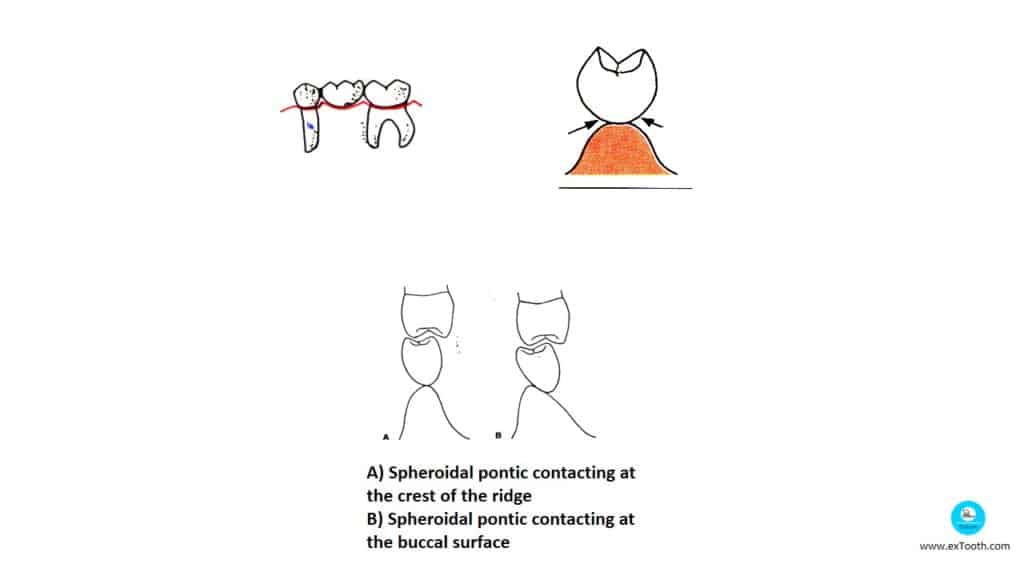
This pontic contacts the tissue only at the ridge crest. They do not have concave gingival surfaces
They are indicated for cases with reduced inter-arch space, the pontic should give the appearance of an exaggerated occlusogingival dimension.
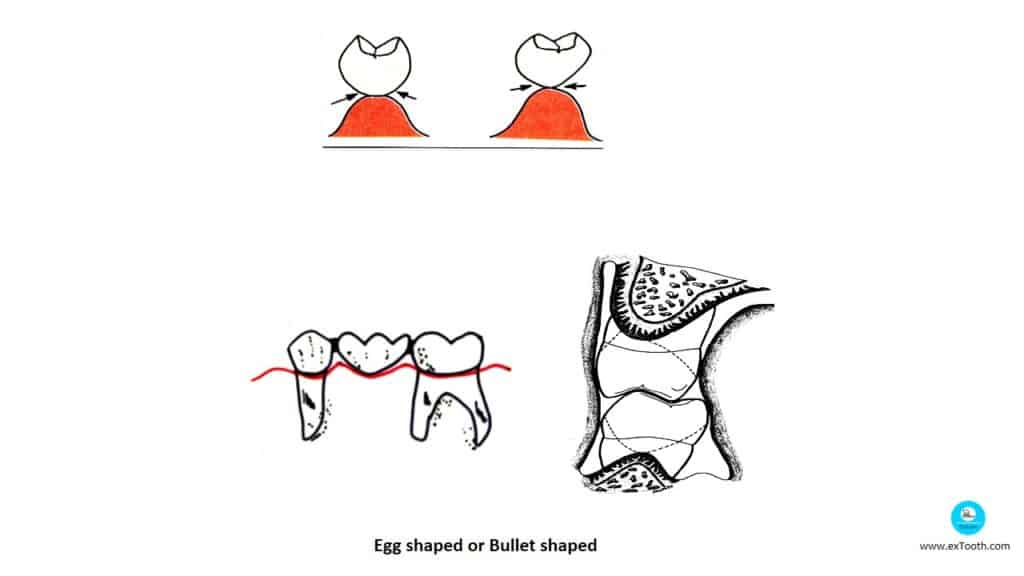
Egg shaped or Bullet shaped
Advantage
– Provides access to oral hygiene procedure.
Disadvantage
– Blocks self-cleansing mechanism of tongue and cheeks.
This pontic has a convex tissue surface, which contacts the tissue at one single point without any pressure.
This is very easy to wash and keep.
The only disadvantage of this design is its poor aesthetics, which results due to wide embrasures. It is indicated for the replacement of mandibular posterior teeth where aesthetics is not a major concern.
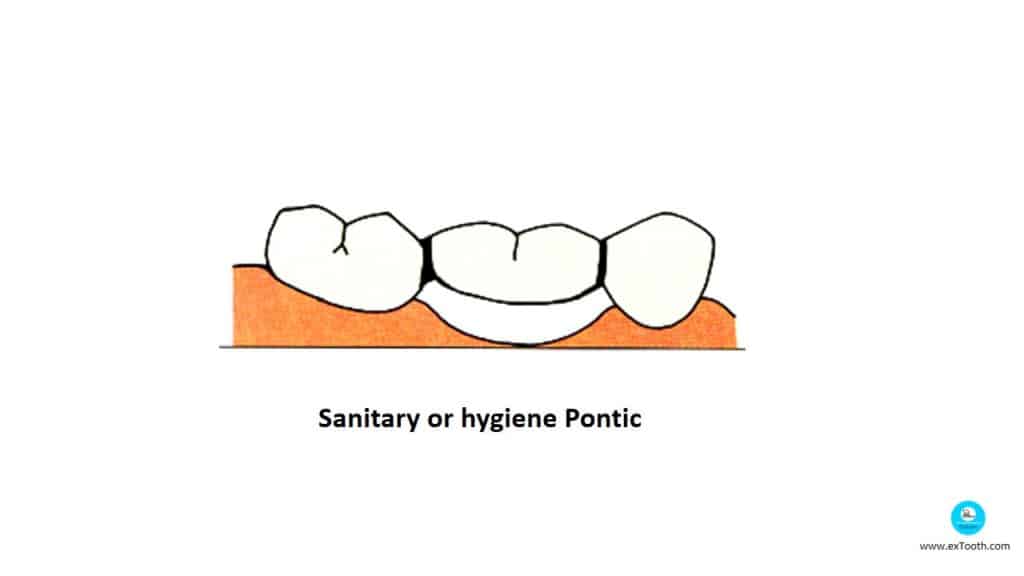
Sanitary or hygiene Pontic
It was introduced by Tinker in 1918
Eissmann H F 1971 fulfills the prerequisites for maintaining a healthy periodontium- doesn’t come in contact with underlying soft tissue, ease access for oral hygiene aids to clean abutment teeth.
It was introduced by Tinker in 1918
The gingival surface of the pontic is convex both buccolingually and mesiodistally.
Features
1. Restores function and stabilizes adjacent with opposing teeth.
2. Made entirely of metal if esthetics is not important.
3. Occlusogingival thickness of pontics should be no less than 3mm and adequate space below it for cleansing.
4. Made of all convex configuration
5. Also called “Fish Belly Appearance”
Advantage
– Easy to maintain oral hygiene.
Disadvantages
– Food entrapment leads to tongue habits.
– If space between gingival surface of pontic and ridge is less may lead to tissue proliferation.
Bar sanitary pontics – These pontics have a flat gingival surface that has sufficient gingival clearance.
Modified Hygienic Pontic
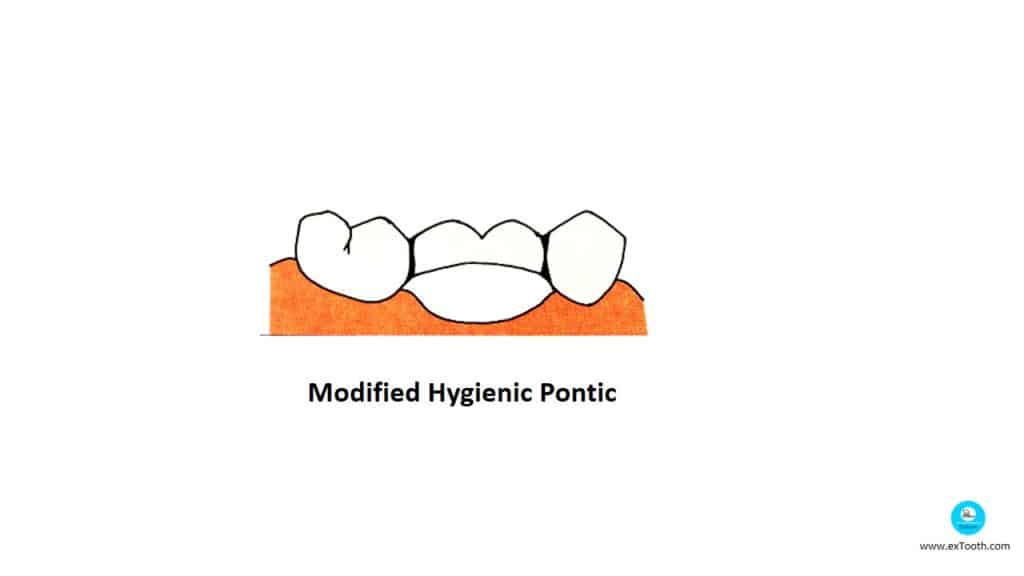
Features
- Gingival surface is shaped like arch may mesiodistally.
- Hyperbolic parabolic appearance.
- Added bulk for the strength of connectors is increased.
- Stress concentration is reduced.
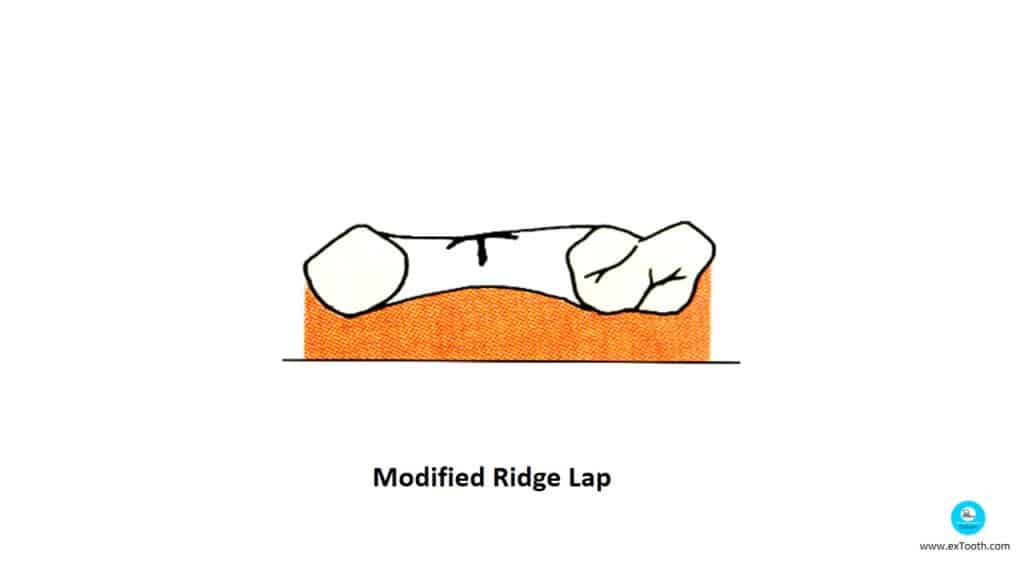
Modified Ridge Lap
- Commonly used in esthetic zone.
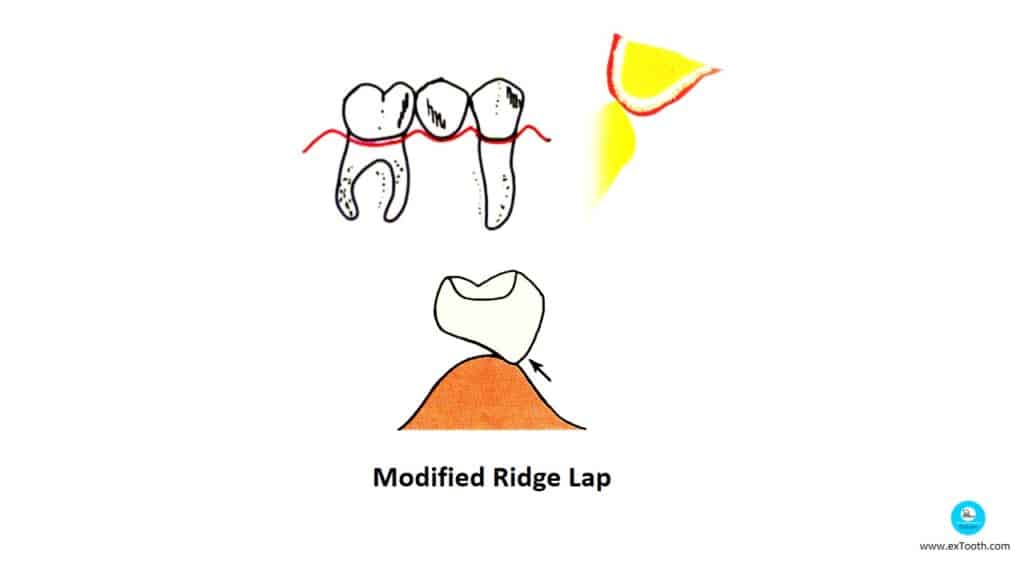
Features
Possess all or nearly all convex surface.
Lingual surface has slightly deflective contour.
Tissue contact narrow faciolingually.
Tissue contact is passive and extend no further lingually than the midline.
Tissue contact area of pontic is passive.
Modified ridge lap pontics where tissue contact is strictly limited to the labial surface of the ridge
Stein R S 1966 , Cavazoz E 1968 : the convex basal surface , which rests on small area on alveolar ridge , fulfills the recommendations made in dental literature with regard to hygiene procedures and prevention of irritation of underlying soft tissues.
Studer S 1997 stated that because of lack of interdental gingiva , open interproximal spaces appear , thus increasing exchange of saliva and air , presents a high risk of food impaction.
Tripodakis A P 1990 : Contour of alveolar ridge requires a convex basal seat in the design of pontic to prevent the impairment of esthetics , function , phonetics.
Tissue surface of the pontic shows a ‘T’ shaped contact. Contact with the facial /buccal surface of the ridge is essential to provide a natural appearance.
Ridge Lap
Features
- Replaces all contours of missing tooth.
- Contacts with the ridge extends beyond midline.
- Has concave filling surface.
Disadvantages
- Impossible to maintain hygiene.
- Causes tissue inflammation and hence not used.
Ridge lap pontic in which tissue surface is inaccessible to cleaning devices.
Council of dental materials and devices 1975 stated that a reduction of surface area doesn’t significantly improve hygiene underneath the pontic – basal contour remains concave .
Root Extension Type
Features
- Extends into the socket.
- Tissue surface is convex and dictated by the shape of the extraction bucket.
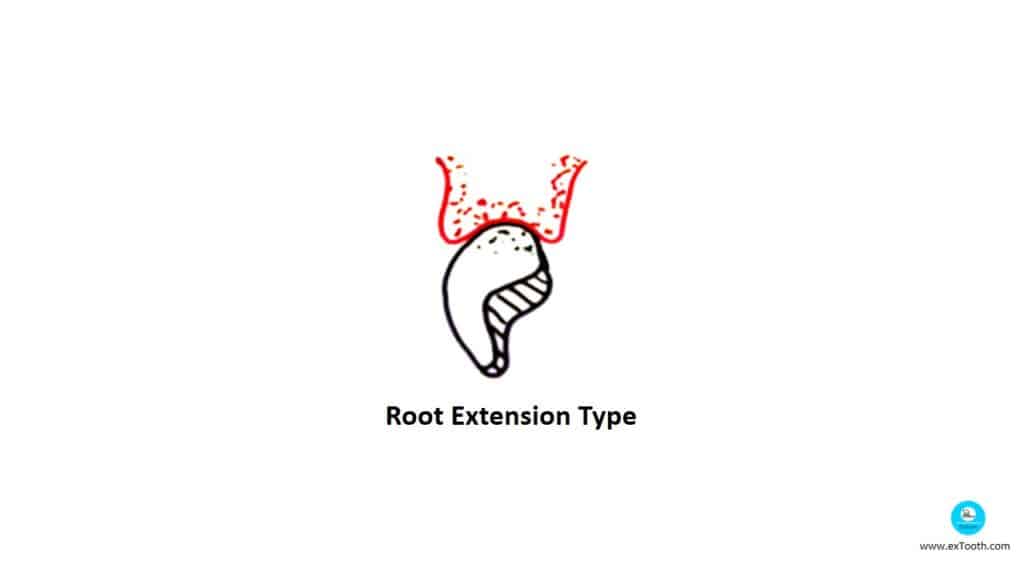
Advantage:
Good esthetic appeal.
Disadvantages:
- Promotes ridge resorption.
- Hinders oral hygiene and wound healing.
Conical Pontic
Tinker 1918 named it “Sanitary Dummy” pontic.
This pontic has a convex tissue surface, which contacts the tissue at one single point without any pressure. This pontic is very easy to clean and maintain. The only disadvantage of this designs its poor aesthetics, which results due to wide embrasures. It is indicated for the replacement of mandibular posterior teeth where aesthetics is not a major concern.
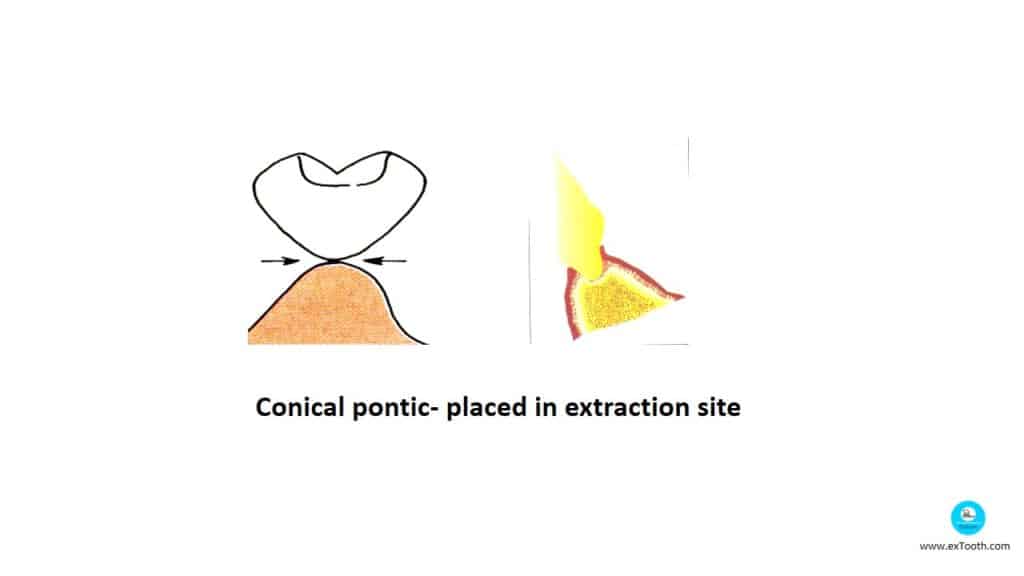
Conical pontic- placed in extraction site
Features:
- Round and cleanable but tip is too small in relation to overall size of the pontic.
Indication:
- Mandibular ridge in non esthetic zone.
Disadvantage:
- Large angle embrassure spaces around tissue contact collect debris.
- Study by Reichenbach E 1931 stated that it was used to prevent the extraction site from collapsing after removal of a tooth and to imitate the natural emergence profile of the tooth.
- Reichenbach E 1931, Dewey K W 1933 also stated that after extended periods of service the adjacent soft tissue tends to become inflamed, and the alveolar bone is resorbed.
- Bodirsky H 1992, Spear F M 1999 also stated that immediate pontic technique can be used as a modified application, to maintain the topography of alveolar ridge after the extraction of the tooth.
Ovate Pontic
Deeway and Ingsmith 1933.
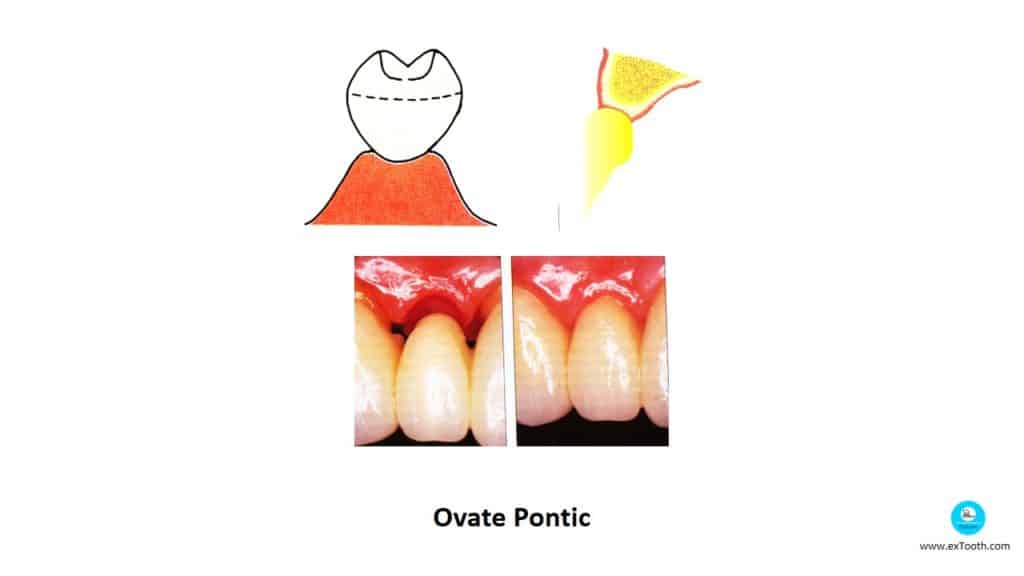
The pontic is designed such that its cervical end extends into the defect of the edentulous ridge. The pontics should be reduced as healing progresses. This pontic is more aesthetic as it appears to arise from the ridge like a natural tooth.
Features:
Tissue contacting is rounded bluntly and set in concavity of the ridge.
Ovate pontic
Concavity is created using provisional restoration and also surgically.
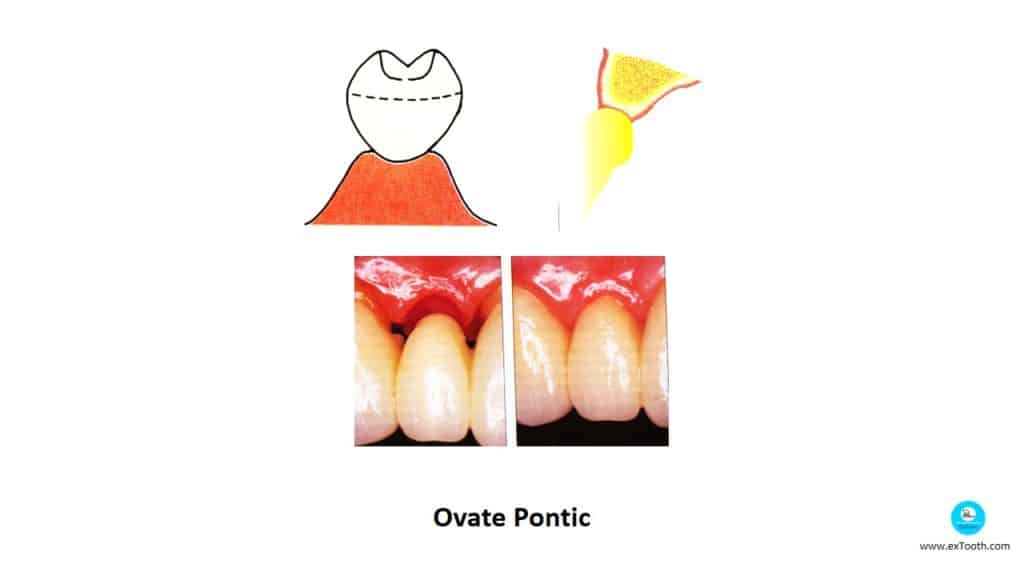
Indication:
Used in broad flat ridges.
Ovate pontic-appears to emerge from gingiva like a natural tooth.
Stein RS 1966- Stated that pressure free contact over a small area produce highly esthetic results in contrast to classic requirements for pontics as this design produces an emergence profile looking similar to that of the natural tooth.
Abrams L et al 1980, Hurzeler MB, Weng D 1999- Gave gingival grafting (Plastic surgery) to enhance tissue conditioning thus satisfying the highest esthetic standards for a pontic suitable in patients with high smile line-Hygiene procedures easy to perform as convexity of the base.
Bodirsky H et al 1992, Spear FM 1999- Gave immediate pontic technique ranging from controlled regeneration directly after tooth extraction.
Inzoma Pontic/Framework full coverage pontic
- Reinforced porcelain system.
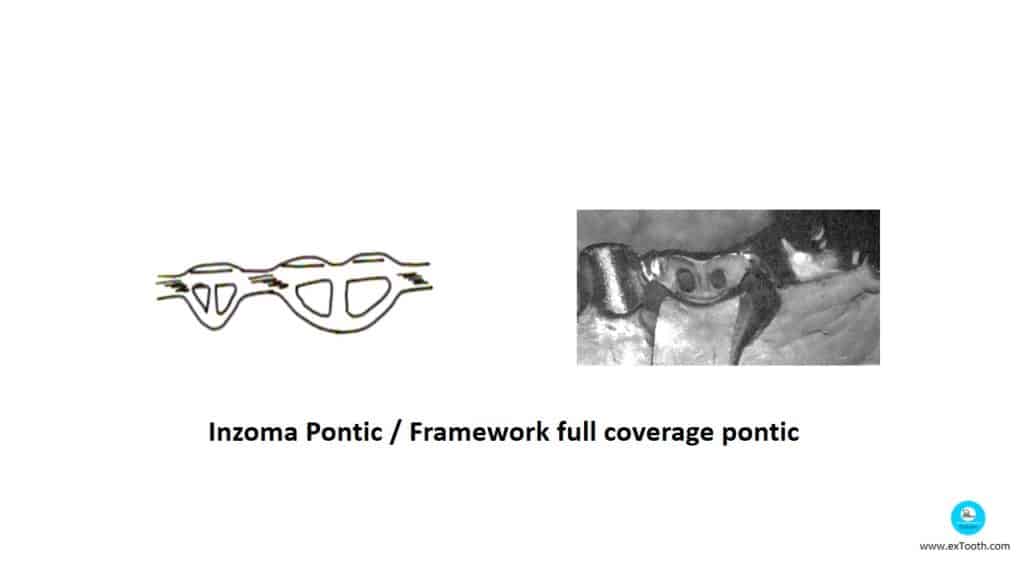
Features:
- Metal design to a interconnecting bar structure.
- Made of occlusal shelf a trim, gingival bar and connector.
Advantages:
- Has good high impact strength and sheer strength].
- Increased load bearing capacity by 55%.
- Use of precious metal is saved because of framework.
An innovative revolutionary Inzoma pontic
Prefabricated Porcelain Facing
Steele’s Interchangeable Facing –.

Whiteside 1959.
Used mainly in lower anterior region, due to excess calculus deposition induced by salivary duct openings.
Porcelain is supported by metal placed at right angle to the occlusal force.
Facings are supplied with standardized metal backings with male plug which fits into female groove on lingual aspect of facing.
Plain Long Pin Pontic
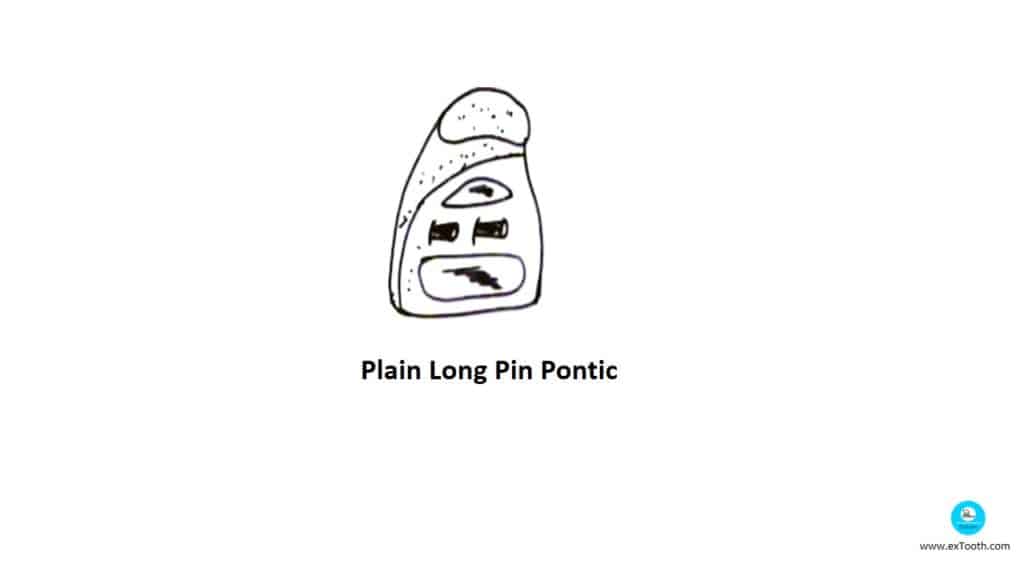
To these facings, the gingival area is again built with porcelain and glazed for tissue tolerance.
Pin pontic modification of long pin pontic, is intend to grind the tissue surface for appropriate contact and then polished or glazed.
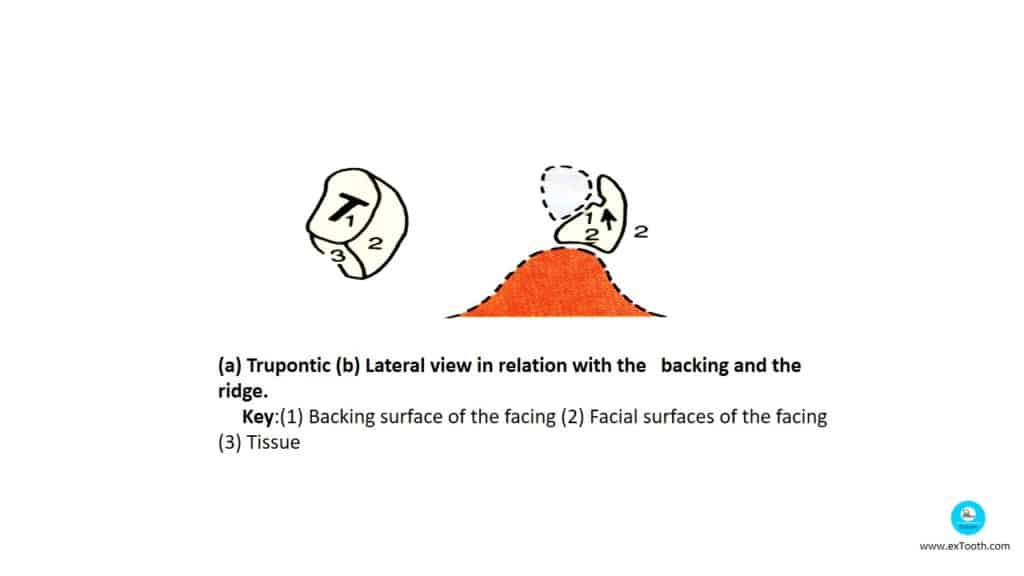
Tru Pontic
This pontic consists of a large gingival bulk, which can be adapted to the ridge. It has a horizontal tubular slot running in the centre of the lingual surface of the facing. It has two proximal slopes/bevels on either side of the central bulk. This slot and the proximal bevels provide retention.
It is indicated in cases with limited inter-arch distance. It cannot be used when there is reduced interocclusal distance due to the presence of a large gingival bulk
- Facing and backing available with the gingival backed tip.
- Cannot be used in decreased occlusogingival height.
- Horizontal tubular slot in the facing runs from centre to lingual side.
Interchangeable facing or flat back facing
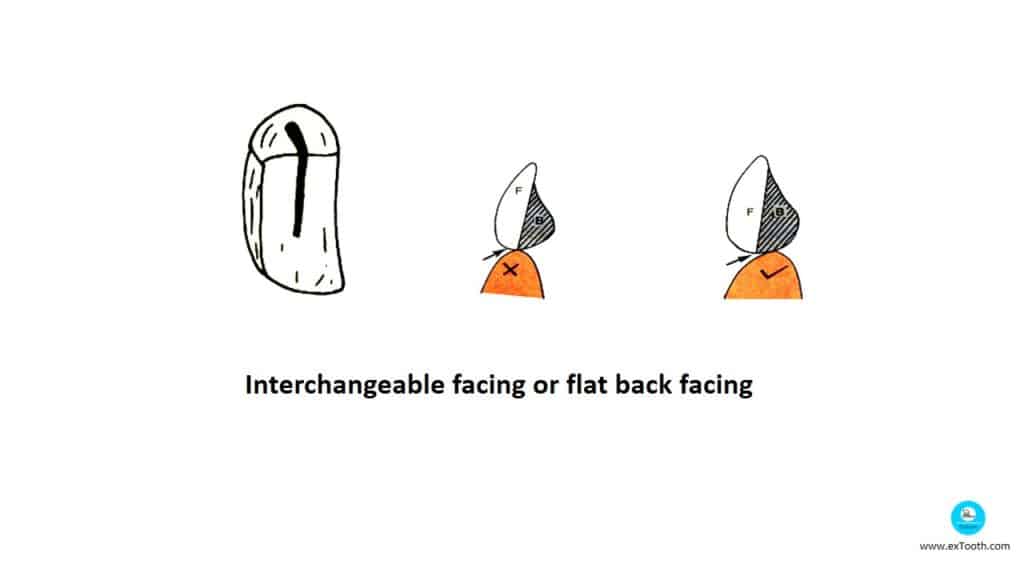
It consists of a vertical slot in its flat lingual surface. The facing is retained by a backing with a lug (elevation), which is designed to engage the retention slot The tissue contact should be a part of the backing (not the backing facing junction) to ensure a smooth finish. The major disadvantage of this system is its complex design, which leads to accumulation of plaque and gingival inflammation.
Tissue contact should be made by the backing and not the facing backing junction
Sanitary facings
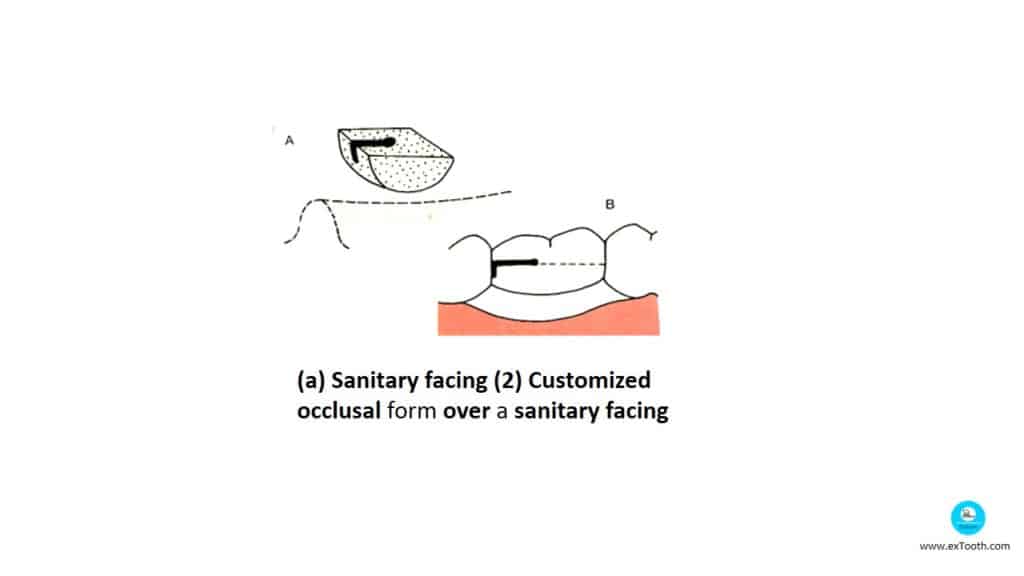
These are prefabricated pontic facings, which resemble sanitary pontics described before. These pontics have slots on the proximal surface to fit into the metal projections made in the fixed partial denture. The facing has a flat occlusal surface which is customized as needed.
Pin facing
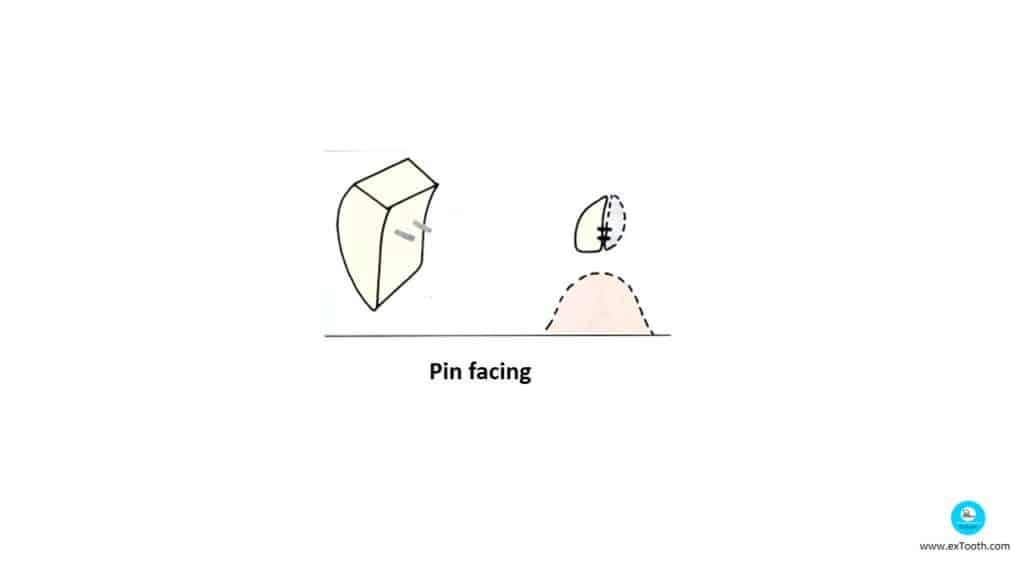
The lingual surface of this facing is flat and consists of two pins for retention. It should be positioned over the backing such that the gold porcelain junction does not contact the tissues. It is indicated in cases with reduced occluso-gingival height.
Modified pin facing
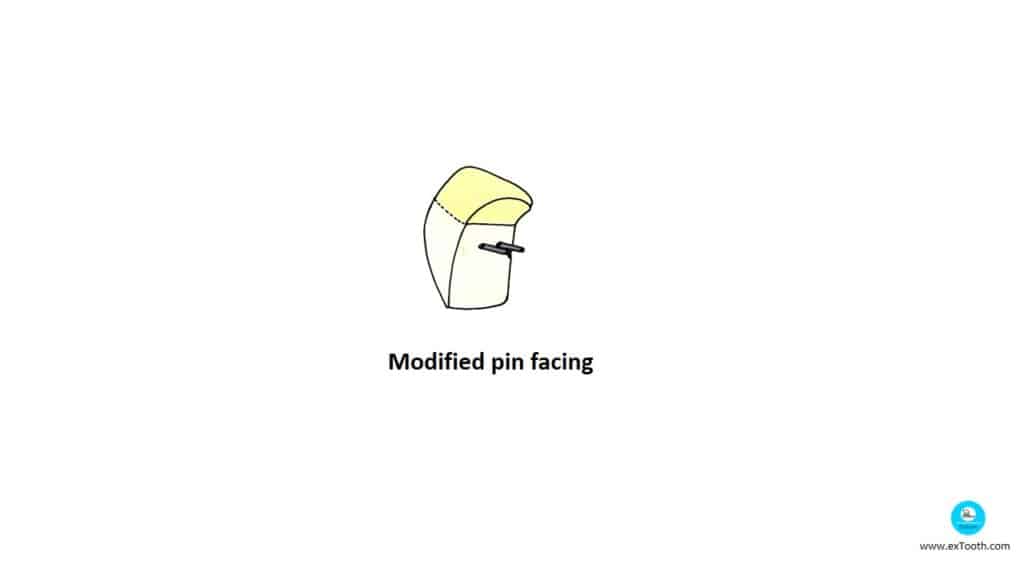
- Here, the flat lingual surface of the pin facing is modified by adding additional porcelain onto the gingival portion of its lingual surface.
- They differ from Harmony facings (discussed later) in that the entire gingival portion of the facing is custom-made.
Reverse Pin Facing
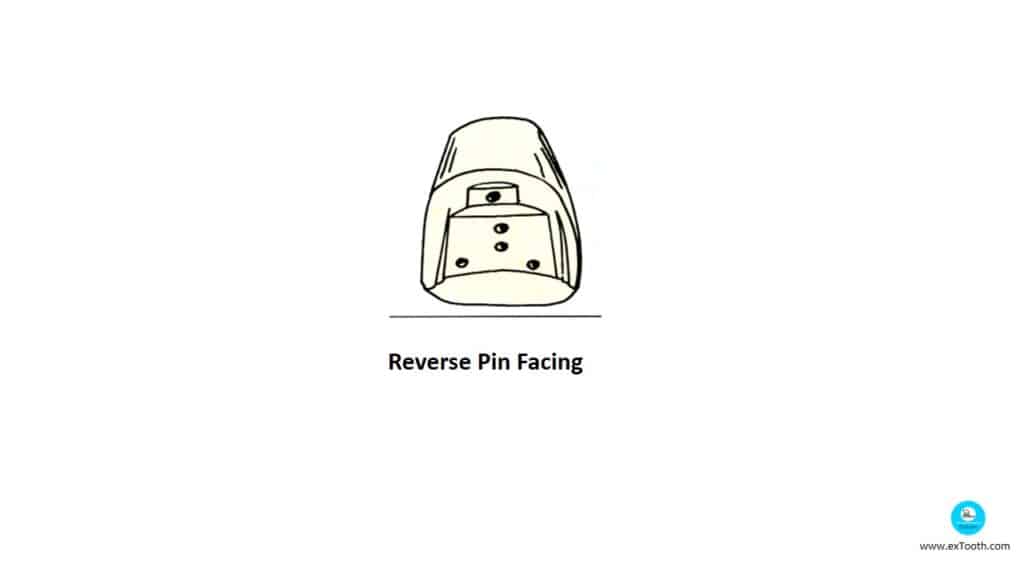
- Pontic facing was made of porcelain denture teeth multiple drill holes of 2mm deep were made using frill press on the lingual surface of the facing.
Pin’s come out of backing, which was cast after building wax in those holes which were attached to the cast ponticDisadvantage:
– Pin holes were stress points that lead to fracture.
Commercially available porcelain denture teeth with pins can be altered to obtain this facing. The pins in the porcelain tooth are ground off and the tooth is altered and customized according to the ridge. Precision drill holes are made on the lingual surface of the facing and these act as source of retention. Nylon bristles are aligned to the drill holes and incorporated into the wax pattern of the backing (here the backing is fabricated according to the facing). It is indicated for cases with deep overbite where short pins are required.
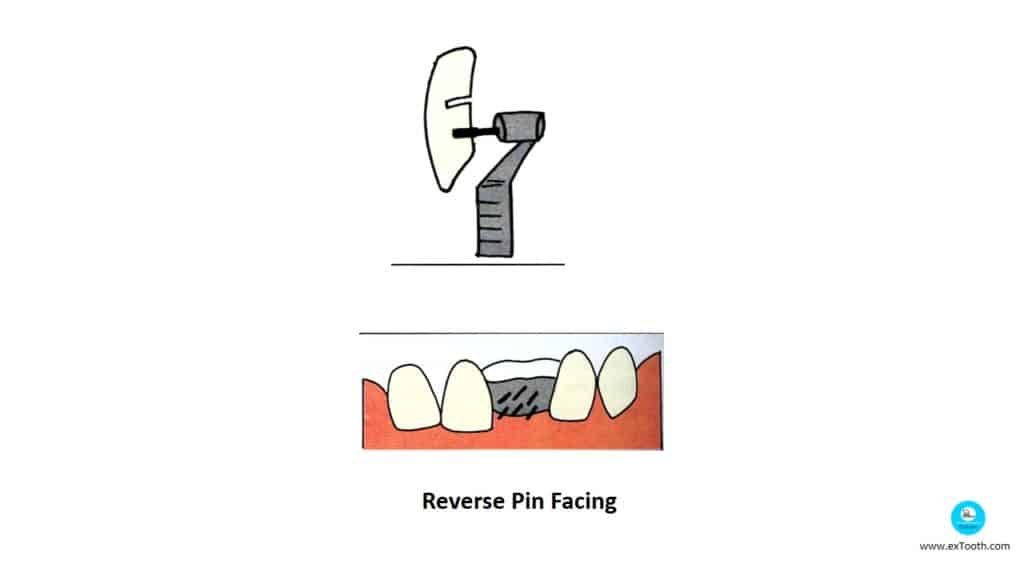
Backing with retentive pins to accept a reverse pin facing
(The pins in the backing are fabricated according to the facing and not the vice versa).
Harmony pontics
They are supplied with an uncontoured porcelain gingival surface and usually with two retentive forms on lingual side.
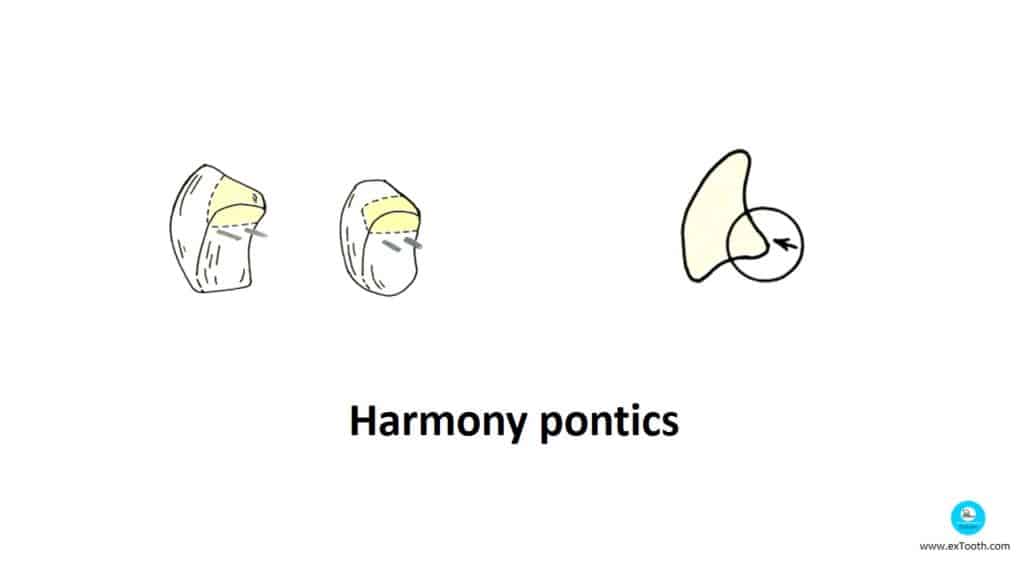
The facing consists of a flat lingual surface with two retentive pins. The gingival surface is usually supplied uncontoured. Porcelain is added to the gingival surface and contoured according to the ridge, finally glazed and finished. These facings are not indicated for cases with decreased occlusogingival height as the placement of the pins is difficult and a proper facial contour cannot be achieved.
It should be remembered that the entire gingival bulk is custom fabricated in a modified pin facing whereas in a harmony facing a portion of the gingival bulk is custom fabricated.
Only a portion of the gingival bulk is contoured in a harmony facing
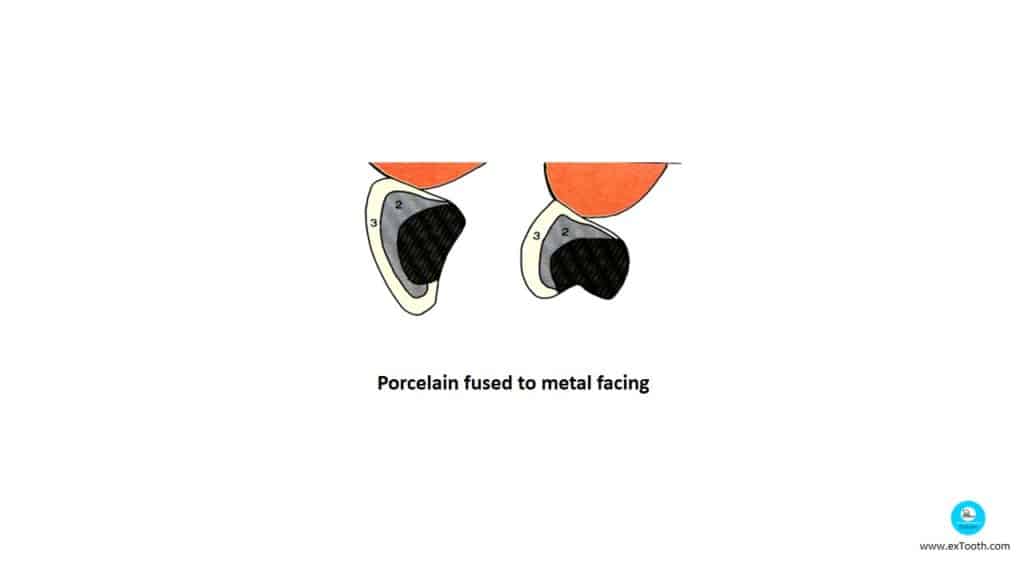
Porcelain fused to metal facing
This facing consists of a metal core over which porcelain is fused to closely resemble the contours of a natural tooth. Care should be taken to avoid contact with the metal porcelain junction with the tissues. It is more aesthetic; hence, it is indicated for anterior teeth. These facings are used when the tissue contact of the pontic should of glazed porcelain.
The pontic has a convex gingival surface that favors pinpoint tissue contact. It is attached to the backing occlusally with the help of retentive pins. The occlusal surface is customized over the backing. They resemble sanitary facings but they have positive pinpoint tissue contact.
Pontic Modification
If the edentulous ridge is heavily resorbed, then the large gingival embrasures between the pontic(s) and retainer(s) will appear highly unaesthetic. These large embrasures or so-called ‘black triangles’ act as a source of plaque accumulation and flossing interference.
Such cases can be treated by two methods:
One is to modify the pontic and fill the entire embrasure space with pink porcelain. This can be done in aesthetically low profile areas like lower anteriors and upper posteriors.
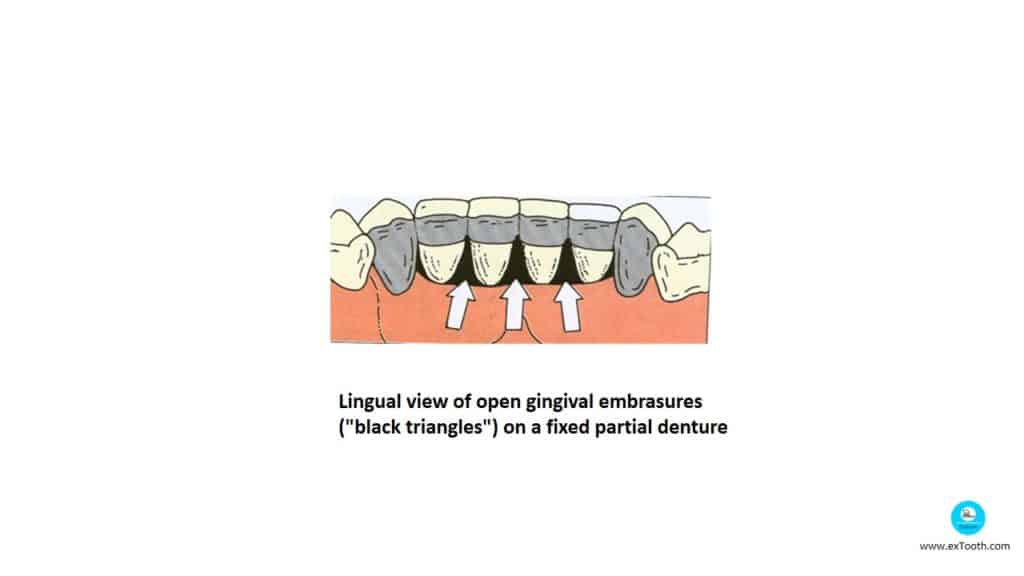
Lingual view of open gingival embrasures
(“black triangles”) on a fixed partial denture
Porcelain fused to metal facing
(1)Metal-backing
(2)Metal of the facing
(3)Ceramic fuse to metal of the facing
Resin Veneered Pontic
Resin Veneered Pontic:
Eg: T-Flex backing and pontics.
Advantages:
a. Manipulation is easy.
b. Inexpensive and easy to repair.
c. Simple procedure.
d. Improved retention.
Disadvantages:
1. Low resistance to abrasion.
2. Lack of dimensional stability.
3. Discoloration.
When opposing natural dentition and complete or partial denture resin veneered teeth are used
All Metal Pontics
- Main advantage is increased strength, fever laboratory steps used in high stress, mandibular posterior region and even in bruxist.
- Poor esthetics.
Metal Ceramic Pontic
- They have a wider scope and most commonly used and widely accepted.
Advantage:
– Strong, easy to clean, good esthetics and biocompatible.
Disadvantage:
– Mechanical failure due to improper framework.
– Not used in long span and high-stress areas.
– Can not be used of occlusogingival space is very less.
They are not used while opposing natural dentition and resin tooth.
Yahoo Guide
1 Jan 2021Youre so right. Im there with you. Your weblog is surely worth a read if anybody comes throughout it. Im lucky I did because now Ive acquired a whole new view of this. I didnt realise that this issue was so important and so universal. You certainly put it in perspective for me.
Webmaster Center
2 Jan 2021Hello.This post was extremely motivating, particularly because I was searching for thoughts on this subject last Wednesday.
Webmaster.m106.com
6 Jan 2021Highly important informations! A big aid and interesting to read! Well done!
www.Japan.M106.COM
12 Feb 2021I am really Glad i found this blog.Added allenchu.4rtofclean.com to my bookmark!
Filozofia
19 Feb 2021Well i’m from Ireland, and throughout Ireland bono and the lads are unquestionably liked and also could certainly not do really much incorrect, we all love them.
USA.XMC.pl
22 Feb 2021Just want to say your article is astounding. The clarity in your post is simply spectacular and i can assume you are an expert on this field. Well with your permission allow me to grab your rss feed to keep up to date with incoming post. Thanks a million and please keep up the fabulous work.
JAPONIA
27 Feb 2021Wow, fantastic blog layout! How long have you been blogging for? you made blogging look easy. The overall look of your site is great, as well as the content!